
Physiological Biomarkers — MCQs

Specificity of a diagnostic test is defined as:
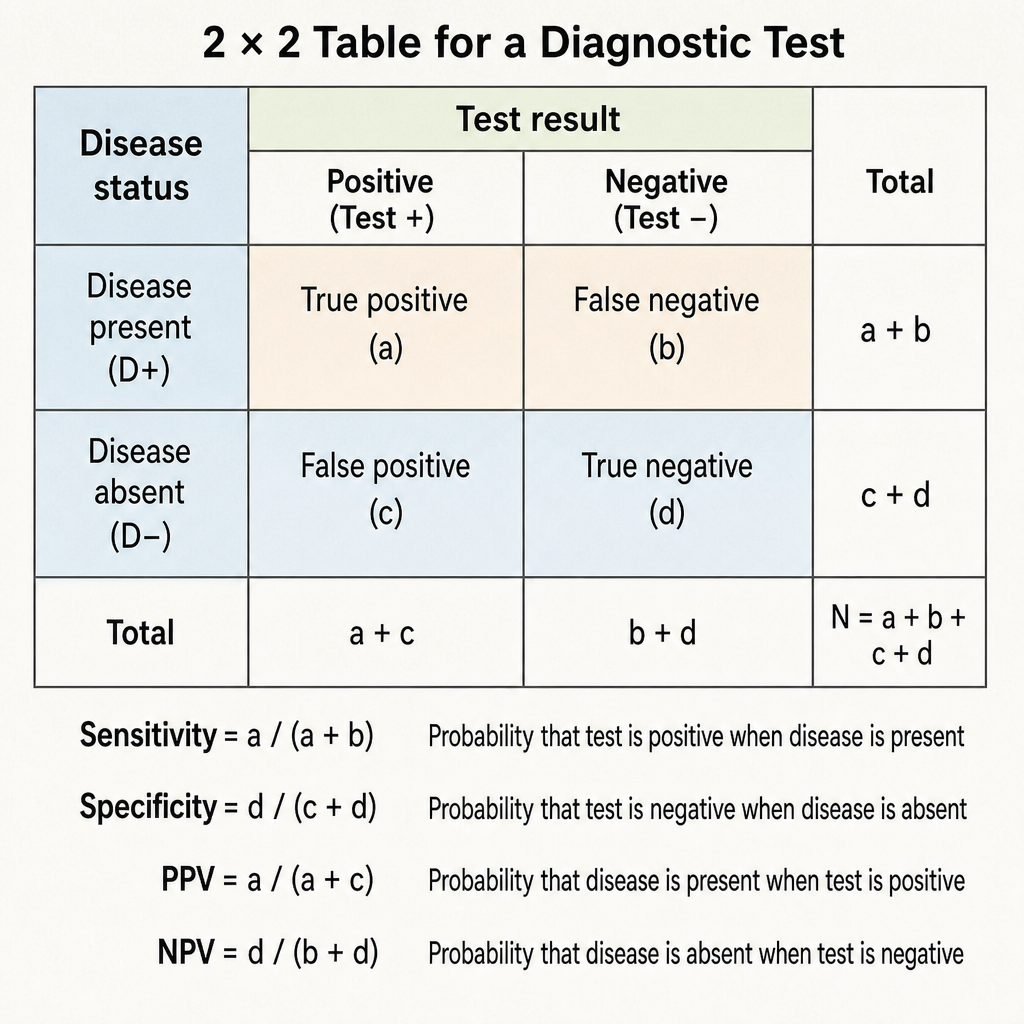
Which of the following best reflects the diagnostic power of a test?
Mr. Murali has 126 mg/dl of fasting plasma glucose. His venous plasma glucose 2h after ingestion of 75g oral glucose load is 149 mg/dl. This patient comes under which stage of WHO diagnostic criteria of diabetes & intermediate hyperglycemia?
What is the most sensitive biochemical marker for a 7-day old myocardial infarction?
Okuda staging contains all except
Cystatin C levels are used for
Procalcitonin is considered a marker for:
Which of the following is the most accurate measure of Glomerular Filtration Rate (GFR)?
What is the recommended daily calcium intake for adult non-pregnant females?
Insulin-like growth factor is secreted by:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app