
General Physiology — MCQs

On this page
Decreased basal metabolic rate is seen in which of the following conditions?
Which of the following hormones is orexigenic?
What is the physiological effect of fever associated with infection?
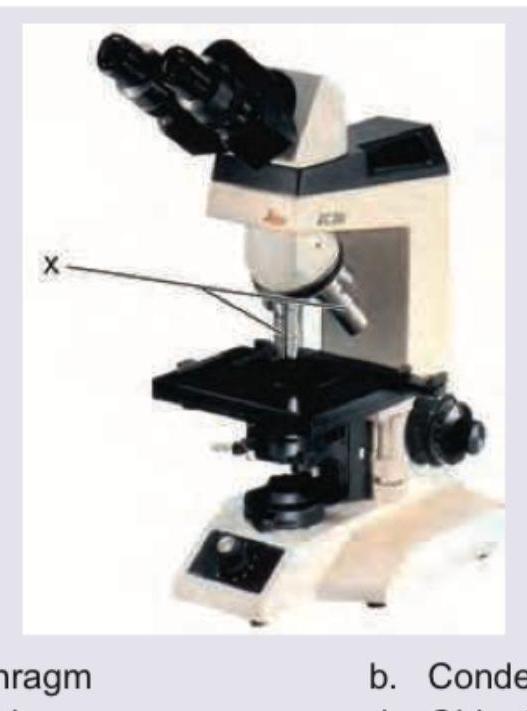
Name the part of the microscope marked as X.
Neural tube defects have which one of the following inheritance patterns ?
All are examples of negative feedback except
DEXA scan of lumbar vertebra and femoral neck are assessed for bone mineral density in menopausal women because of all except
BMR is increased in all except:
Which of the following is a height dependent index?
Which of the following is false regarding suspended animation
Practice by Chapter
Cell Structure and Function
Practice Questions
Membrane Transport Mechanisms
Practice Questions
Bioelectric Phenomena
Practice Questions
Homeostasis and Feedback Mechanisms
Practice Questions
Body Fluid Compartments
Practice Questions
Signal Transduction Mechanisms
Practice Questions
Cell-to-Cell Communication
Practice Questions
Principles of Physiological Measurement
Practice Questions
Osmosis and Osmotic Pressure
Practice Questions
Physiological Adaptation Mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app