
General Physiology — MCQs

On this page
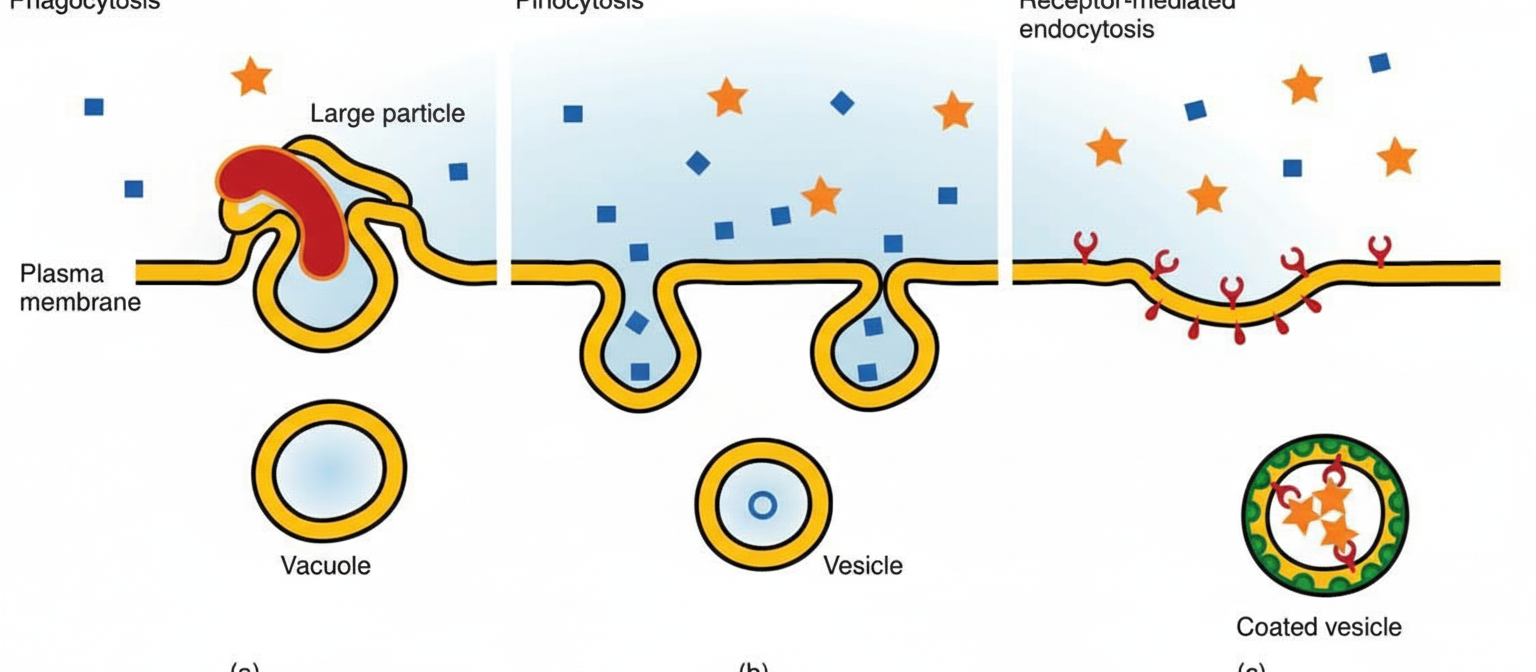
Which statement about the following cellular phenomenon is false?
All are seen more in ECF except?
Pacinian corpuscles transmit which sensation?
What is the approximate protein to lipid ratio in myelin?
What is the main constituent of the plasma membrane?
Inulin is used for the measurement of which body fluid compartment?
All of the following are stress responses except?
Gap junctions are present in?
Which is the efferent neuron for skeletal muscle?
Stem cells are found in which of the following locations?
Practice by Chapter
Cell Structure and Function
Practice Questions
Membrane Transport Mechanisms
Practice Questions
Bioelectric Phenomena
Practice Questions
Homeostasis and Feedback Mechanisms
Practice Questions
Body Fluid Compartments
Practice Questions
Signal Transduction Mechanisms
Practice Questions
Cell-to-Cell Communication
Practice Questions
Principles of Physiological Measurement
Practice Questions
Osmosis and Osmotic Pressure
Practice Questions
Physiological Adaptation Mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app