
General Physiology — MCQs

On this page
What is the diameter of Type C fibers?
The magnitude of the electrical potential difference that exists across a membrane can be determined by which of the following equations?
Which type of muscle exercise involves the muscle changing length against a constant load?
What does the Golgi tendon organ primarily detect?
Oxidative capacity is high in which type of skeletal muscle fiber?
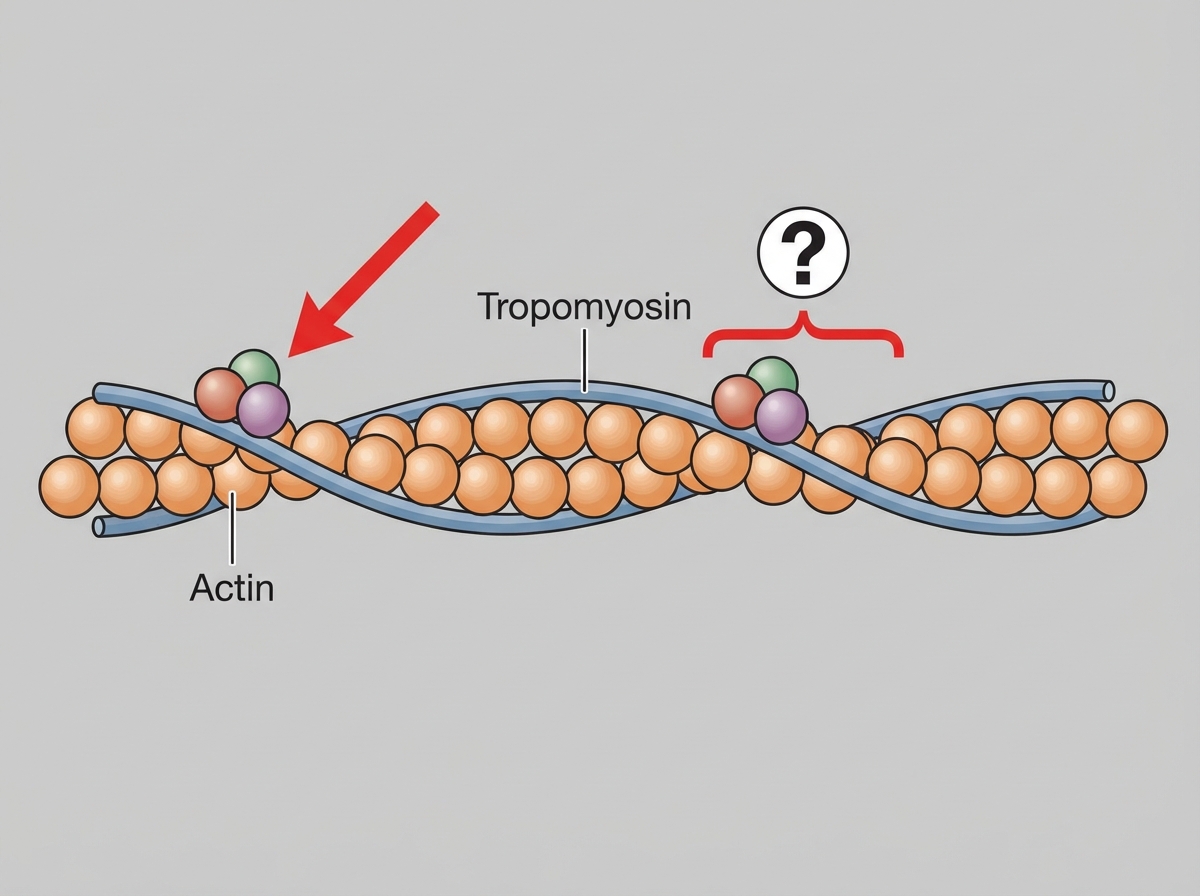
Which protein is shown in the thin filament as illustrated?
Positive feedback is seen in which of the following?
During skeletal muscle contraction, which bands shorten?
Which statement is true regarding Type-2 muscle fibers?
Which of the following statements is true about Nissl granules?
Practice by Chapter
Cell Structure and Function
Practice Questions
Membrane Transport Mechanisms
Practice Questions
Bioelectric Phenomena
Practice Questions
Homeostasis and Feedback Mechanisms
Practice Questions
Body Fluid Compartments
Practice Questions
Signal Transduction Mechanisms
Practice Questions
Cell-to-Cell Communication
Practice Questions
Principles of Physiological Measurement
Practice Questions
Osmosis and Osmotic Pressure
Practice Questions
Physiological Adaptation Mechanisms
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app