
Gastrointestinal System — MCQs

On this page
What is the normal intra-abdominal pressure?
Which of the following actions is attributed to cholecystokinin?
Ascorbic acid is a potent enhancer of iron absorption because it:
What is the most important action of secretin?
What are the final sugars present in intestinal chyme?
Which of the following clinical laboratory observations is suggestive of Maple syrup urine disease?
What is true about gastric acid secretion?
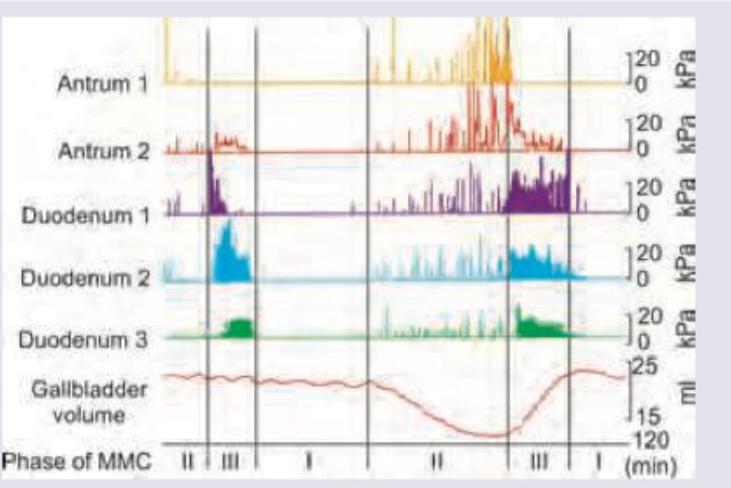
The image shows migrating motor complexes in various parts of gut. Identify the correct statement.
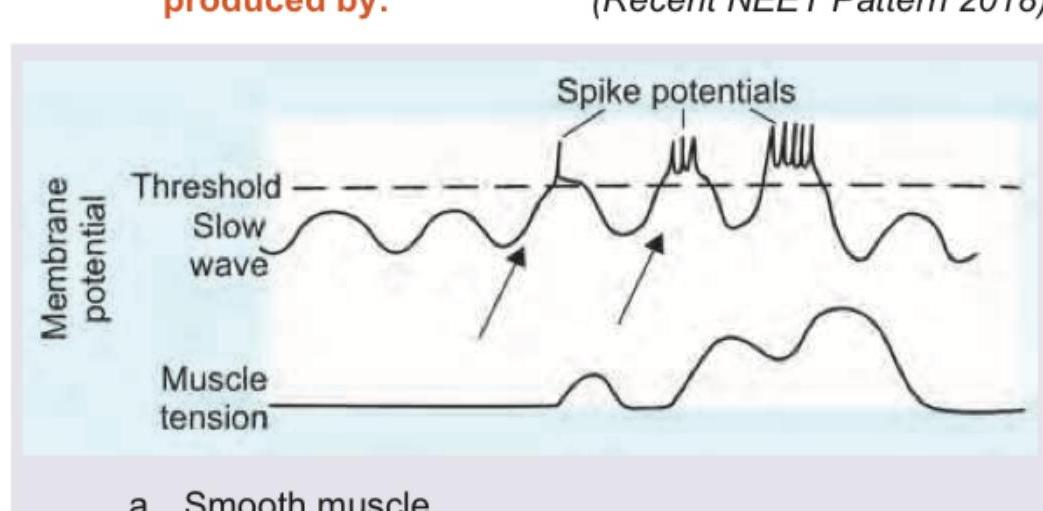
The following marked recordings in GIT are produced by:
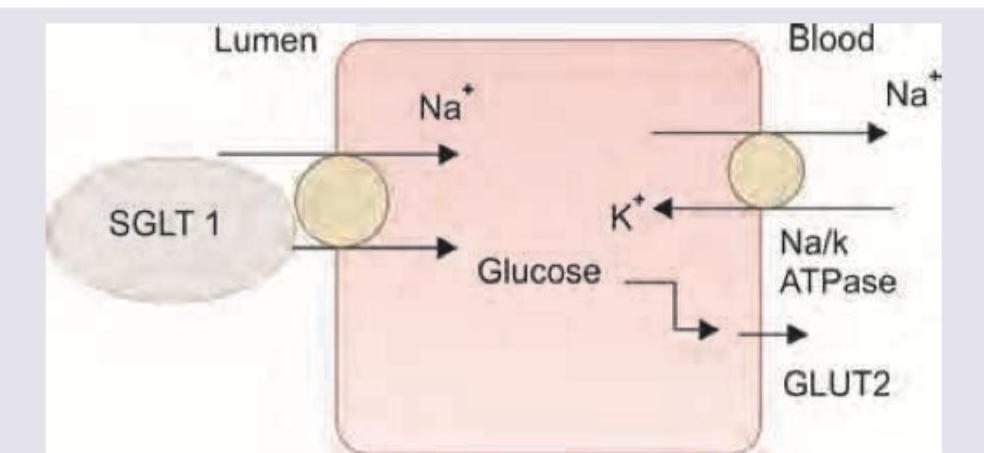
Which of these is true about the highlighted transporter?
Practice by Chapter
Gastrointestinal Motility
Practice Questions
Gastrointestinal Secretions
Practice Questions
Digestion and Absorption
Practice Questions
Gastrointestinal Hormones
Practice Questions
Hepatobiliary Physiology
Practice Questions
Pancreatic Exocrine Function
Practice Questions
Gastrointestinal Circulation
Practice Questions
Intestinal Immune System
Practice Questions
Gut Microbiome
Practice Questions
Regulation of Food Intake
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app