
Gastrointestinal System — MCQs

On this page
Which of the following hormones is orexigenic?
Which of the following cells is responsible for destroying bacterial foreign bodies in liver sinusoids?
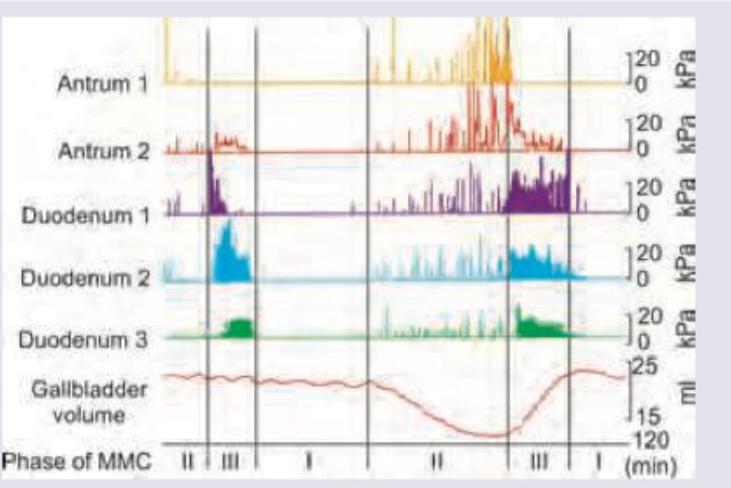
The image shows migrating motor complexes in various parts of gut. Identify the correct statement.
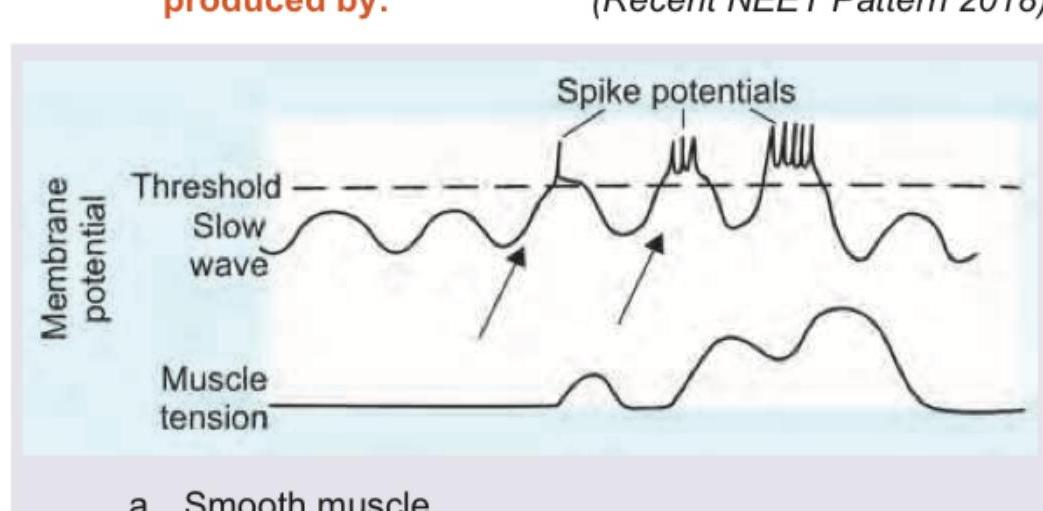
The following marked recordings in GIT are produced by:
Which of the following are functions of the gall bladder? I. Reservoir for bile II. Production of bile III. Secretion of mucus IV. Concentration of bile Select the correct answer using the code given below :
Resection of which part of intestine does not significantly affect fluid and electrolyte balance?
Iron is absorbed predominantly in the
With reference to the role of fibre in diet, consider the following statements: 1. It inhibits faecal mutagen synthesis. 2. It reduces post-prandial glucose. 3. It decreases the transit time of food in the bowel. Which of the above represent(s) the role of fibre in our diet?
Which transporter is responsible for the absorption of glucose in the intestine when a person is given Oral Rehydration Solution (ORS)?
A child presented with dehydration and was supplemented with ORS solution for management. Which of the following transporters help in the absorption of glucose from GIT?
Practice by Chapter
Gastrointestinal Motility
Practice Questions
Gastrointestinal Secretions
Practice Questions
Digestion and Absorption
Practice Questions
Gastrointestinal Hormones
Practice Questions
Hepatobiliary Physiology
Practice Questions
Pancreatic Exocrine Function
Practice Questions
Gastrointestinal Circulation
Practice Questions
Intestinal Immune System
Practice Questions
Gut Microbiome
Practice Questions
Regulation of Food Intake
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app