
Fatigue Mechanisms — MCQs

What are the products of the isocitrate to α-ketoglutarate conversion in the TCA cycle?
Magnesium is not involved in ?
Golgi tendon organs are innervated by which type of nerve fibre?
What is the neurotransmitter primarily involved in muscle contraction?
During a 100 m sprint which of the following is used by the muscle for meeting energy demands?
Which of the following would be least likely seen 14 days after a rat is injected with a drug that kills all of its pancreatic B cells?
Milk production in pregnancy is inhibited by :
What do motor evoked potentials primarily assess?
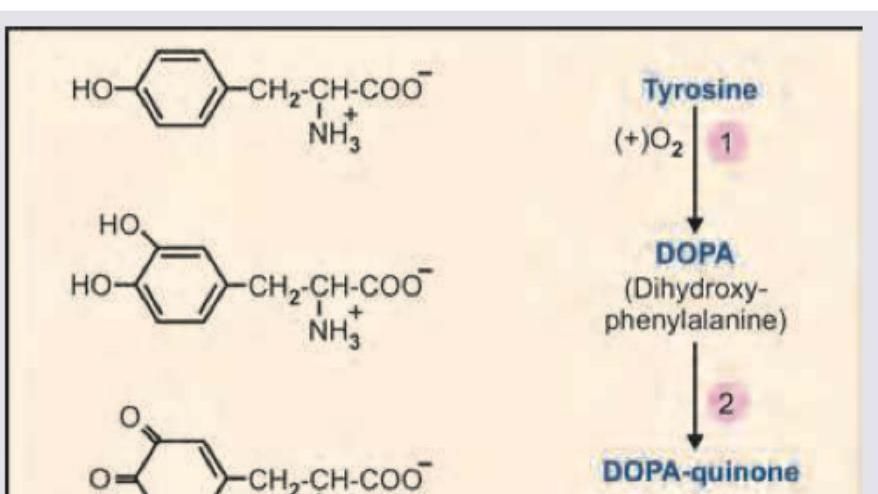
Name the product marked as X in the image shown below:
A 42-year-old firefighter candidate undergoes VO2 max testing showing 32 mL/kg/min (below required 42 mL/kg/min). His body composition shows 28% body fat. He has normal cardiac function (ejection fraction 60%), hemoglobin 15.2 g/dL, and no respiratory disease. Lactate threshold occurs at 65% of VO2 max. Evaluate the most effective evidence-based training strategy to meet occupational requirements within 12 weeks.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app