
Cardiovascular Responses to Exercise — MCQs

Which of the following is a FALSE statement regarding hemodynamic changes occurring during exercise?
Which of the following causes coronary vasodilation?
If the contractility of the heart is decreased, which of the following is seen ?
During heavy exercise the cardiac output (CO) increases up to five fold while pulmonary arterial pressure rises very little. This physiological ability of the pulmonary circulation is best explained by
Concentric hypertrophy of left ventricle is seen in -
Blood supply to the brain during moderate exercise:
During exercise in physiological limits, what is the effect on end systolic volume?
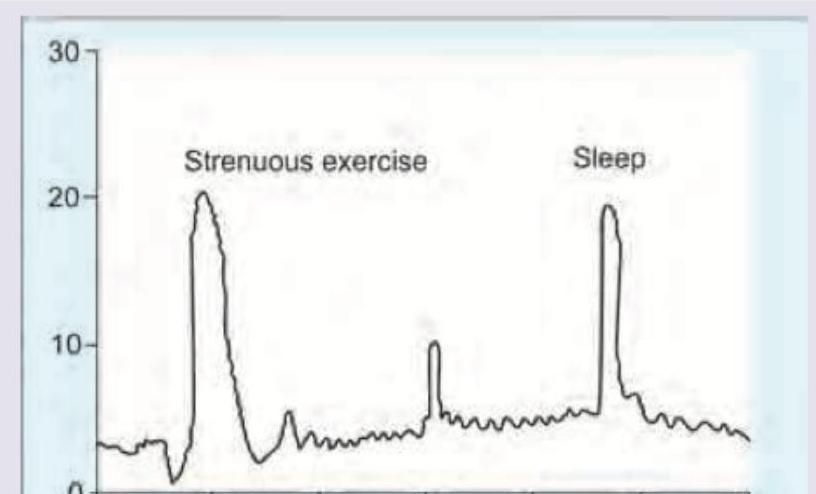
The blood levels of hormones are elevated during exercise and sleep as shown. Which hormone would exhibit this diurnal pattern?
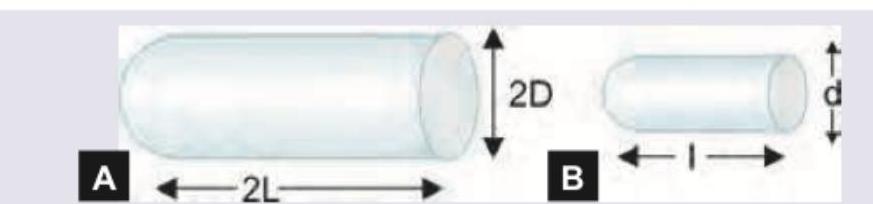
There are two blood vessels shown below. Assuming that pressure along both the vessels is same and both of them follow linear flow pattern, what will be the amount of blood flow in A compared to B?
Cushing reflex is associated with all except?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app