
Endocrinology — MCQs

On this page
Intake of exogenous steroids causes
In a person who has fasted for 5 days, all are seen except:
What is the primary mechanism by which corticosteroids affect calcium levels in the body?
What is the effect of insulin administration on the respiratory quotient (RQ) in diabetes?
Wolf Chaikoff effect:
All of the following statements about insulin-like growth factor (IGF) are true, except which of the following?
What is the primary function of the paraventricular and supraoptic nuclei?
In uncomplicated cases, cortisol levels typically return to normal within how many days after acute hemorrhage?
Osteoclasts are inhibited by:
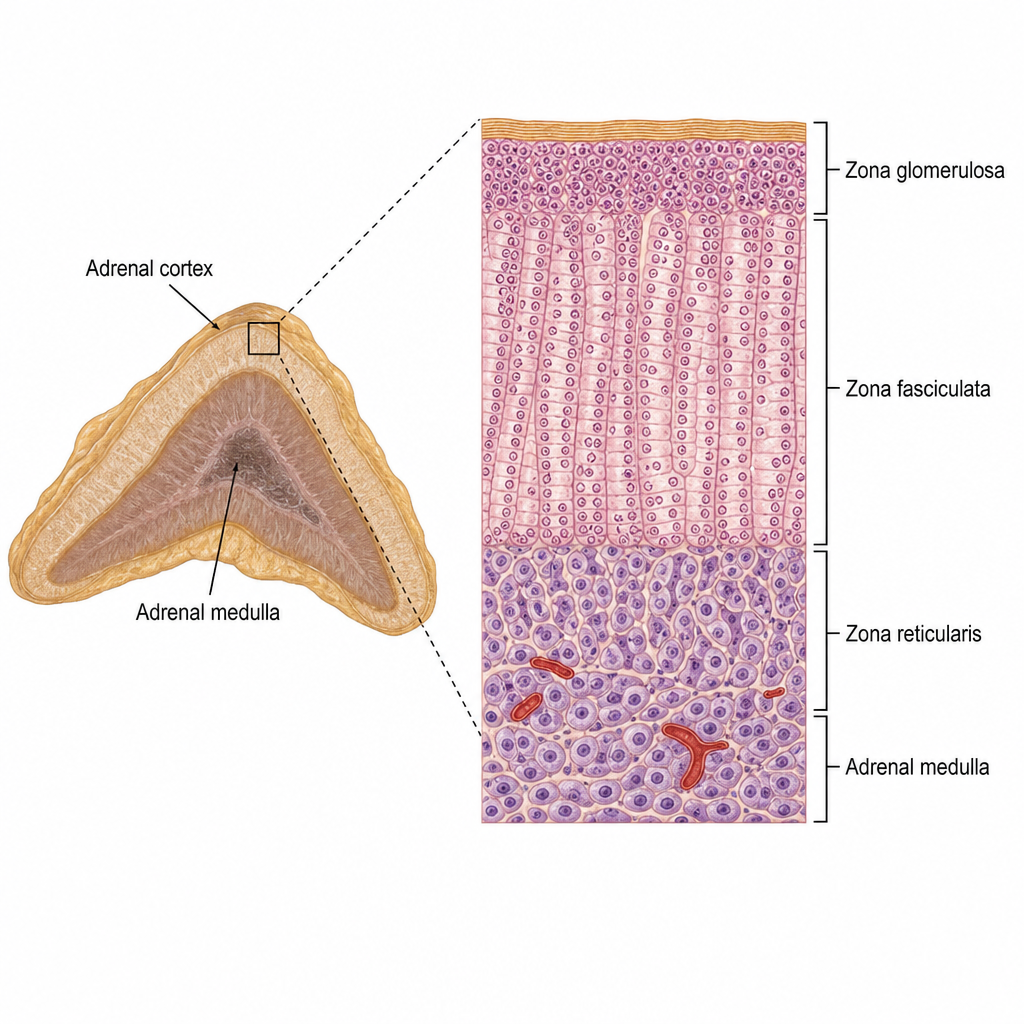
The hormone produced from the area marked in the provided image of the adrenal gland is:
Practice by Chapter
Principles of Endocrine Regulation
Practice Questions
Hypothalamus and Pituitary Gland
Practice Questions
Thyroid Physiology
Practice Questions
Adrenal Cortex and Medulla
Practice Questions
Pancreatic Hormones and Glucose Metabolism
Practice Questions
Calcium and Phosphate Homeostasis
Practice Questions
Growth Hormone and Growth Factors
Practice Questions
Endocrine Regulation of Metabolism
Practice Questions
Hormone Receptors and Signaling
Practice Questions
Assessment of Endocrine Function
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app