
Endocrinology — MCQs

On this page
Hyperpigmentation in Addison's disease is due to increased secretion of:
A woman is diagnosed with a pituitary microadenoma and has elevated serum prolactin levels. She presents with secondary amenorrhea and infertility. What is the most likely mechanism by which hyperprolactinemia causes these symptoms?
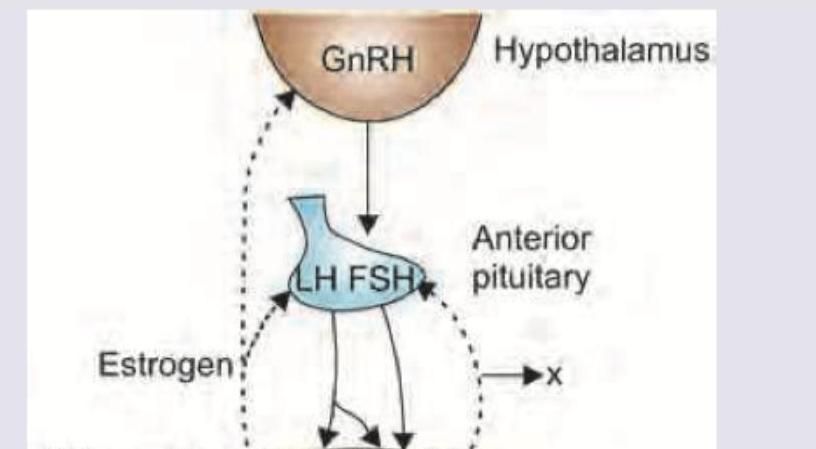
Which of the following is correct about the feedback hormone marked as $X$, secreted by developing ovarian follicles during the follicular phase?
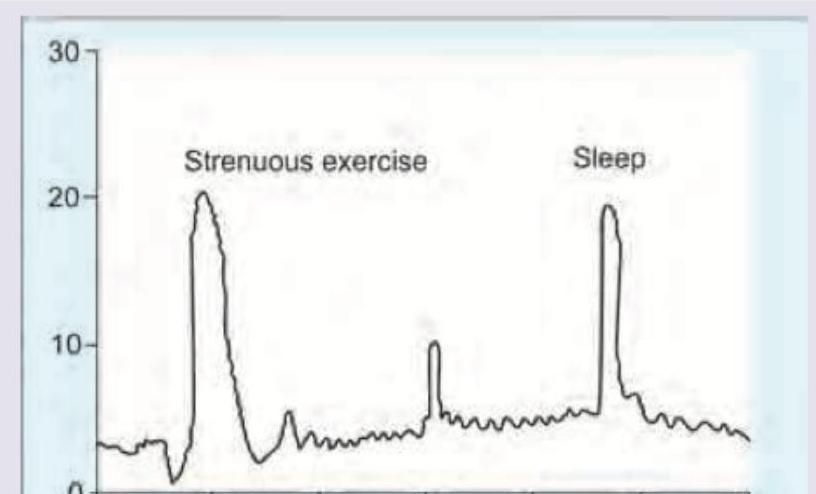
The blood levels of hormones are elevated during exercise and sleep as shown. Which hormone would exhibit this diurnal pattern?
Match List-I with List-II and select the correct answer using the code given below the Lists: **List-I** A. Pineal gland B. Testis C. Adrenal gland D. Ovary **List-II** 1. Testosterone 2. Estrogen 3. Cortisol 4. Melatonin
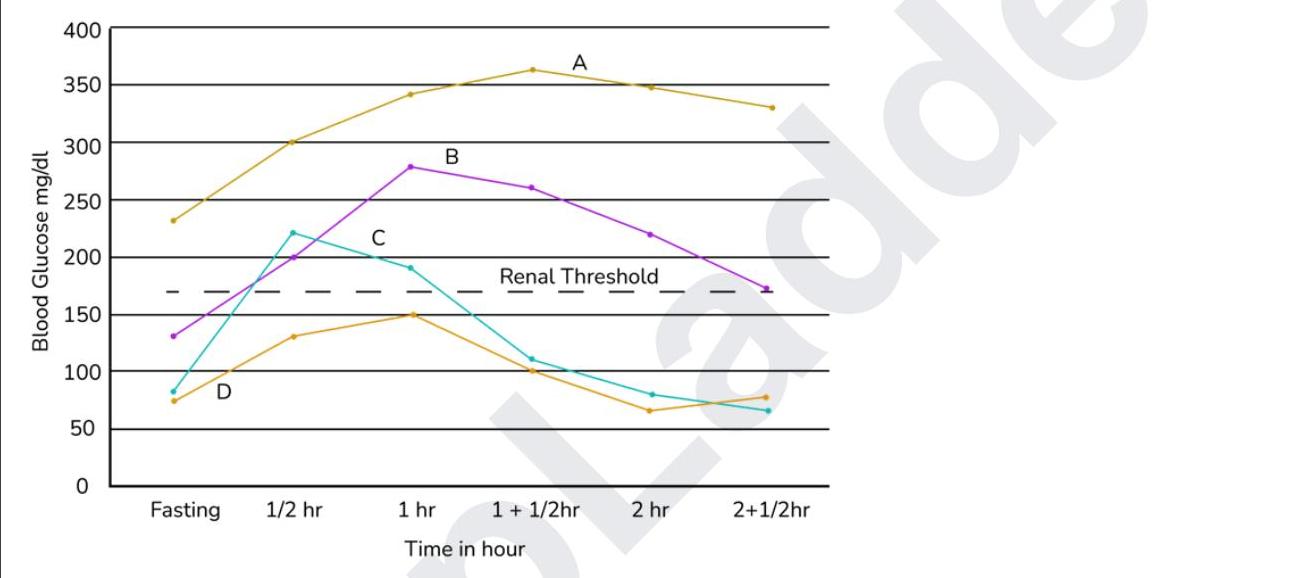
Which of the following represents a normal response to an OGTT?
Which of the following is the primary tissue dependent on insulin for glucose uptake?
Which hormone most strongly stimulates gluconeogenesis during prolonged fasting?
A patient with a pituitary tumor demonstrates elevated prolactin levels. Which of the following changes in dopamine signaling best explains the hyperprolactinemia?
A 20-year-old college student has elevated stress levels due to her rigorous academic schedule, social commitments, and family pressures. She complains of never having enough time for all her responsibilities. Which of the following hormones acts by intracellular receptors to exert the physiologic effects of her stress?
Practice by Chapter
Principles of Endocrine Regulation
Practice Questions
Hypothalamus and Pituitary Gland
Practice Questions
Thyroid Physiology
Practice Questions
Adrenal Cortex and Medulla
Practice Questions
Pancreatic Hormones and Glucose Metabolism
Practice Questions
Calcium and Phosphate Homeostasis
Practice Questions
Growth Hormone and Growth Factors
Practice Questions
Endocrine Regulation of Metabolism
Practice Questions
Hormone Receptors and Signaling
Practice Questions
Assessment of Endocrine Function
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app