
Endocrinology — MCQs

On this page
Reduction in estradiol levels leads to all except?
Increased prolactin is associated with which of the following?
Which of the following is NOT true about thyroxine?
Which hormones are produced by the zona glomerulosa of the adrenal cortex?
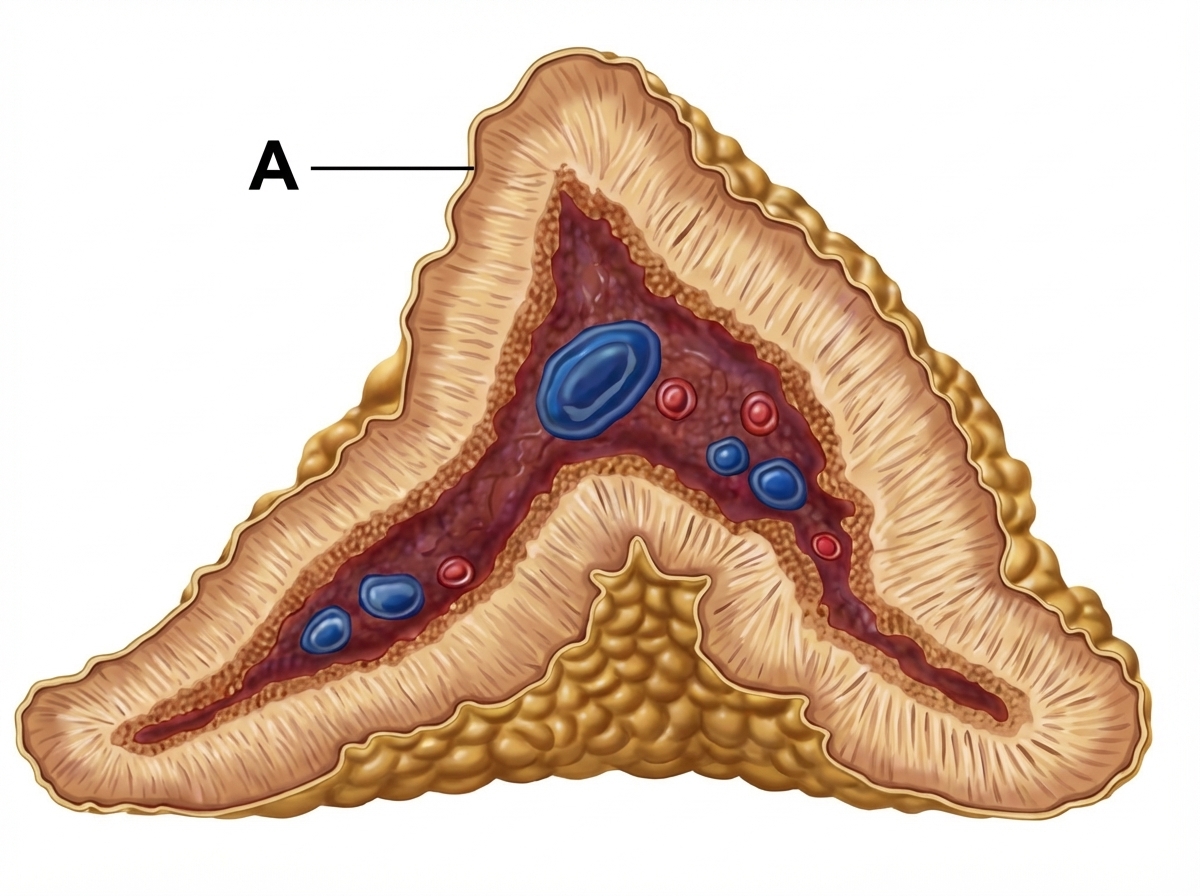
The provided diagram shows the adrenal gland. Identify the hormone produced from the area labeled 'A'.
Which of the following is both synthesized and stored in the hypothalamus?
Obesity is ordinarily associated with low ghrelin levels. Which of the following conditions is an exception where obesity is associated with high ghrelin levels?
All of the following are true about neuropeptide Y EXCEPT:
Which of the following hormones is not secreted by the kidney?
Which of the following hormones increases during sleep?
Practice by Chapter
Principles of Endocrine Regulation
Practice Questions
Hypothalamus and Pituitary Gland
Practice Questions
Thyroid Physiology
Practice Questions
Adrenal Cortex and Medulla
Practice Questions
Pancreatic Hormones and Glucose Metabolism
Practice Questions
Calcium and Phosphate Homeostasis
Practice Questions
Growth Hormone and Growth Factors
Practice Questions
Endocrine Regulation of Metabolism
Practice Questions
Hormone Receptors and Signaling
Practice Questions
Assessment of Endocrine Function
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app