
Electrolytes and Body Fluids — MCQs

On this page
Where is the majority of the body's sodium present?
Prolonged immobilization leads to which of the following conditions?
All are seen more in ECF except?
Calculate the osmolarity of normal saline.
What is the normal route of calcium excretion?
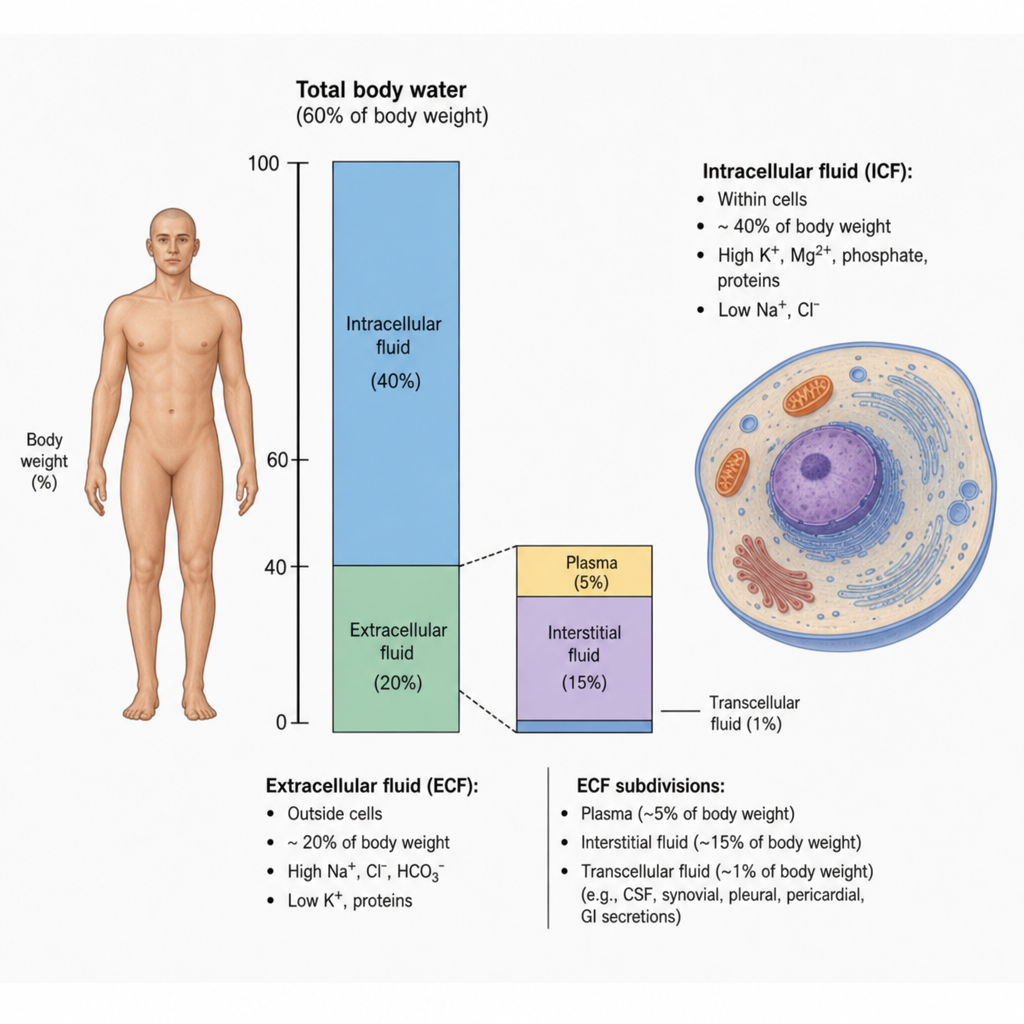
Which of the following statements concerning intracellular fluid is true? 1. The intracellular fluid constitutes approximately 40% of the total body weight. 2. Sodium is the primary cation of the intracellular fluid. 3. The intracellular fluid contains higher concentrations of proteins and phosphates compared to the extracellular fluid.
What is true about hyperkalemia?
Which ion is least common in End-of-Functional-Test (EOF)?
Hyperkalemia can occur in all of the following conditions, except?
Where are osmoreceptors located?
Practice by Chapter
Body Fluid Compartments and Composition
Practice Questions
Osmolality and Tonicity
Practice Questions
Sodium and Water Balance
Practice Questions
Potassium Homeostasis
Practice Questions
Calcium and Phosphate Regulation
Practice Questions
Magnesium Metabolism
Practice Questions
Fluid Shifts Between Compartments
Practice Questions
Edema Formation Mechanisms
Practice Questions
Dehydration Physiology
Practice Questions
Disorders of Electrolyte Balance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app