
Electrolytes and Body Fluids — MCQs

On this page
What is the normal plasma osmolality range in humans?
Osmotic adaptations are all except:
Edema is visible when the amount of fluid accumulated is:
1.5 mL of a solution containing 20 mg/mL of Evans blue dye is injected into plasma. If the final concentration of the dye is 0.015 mg/mL, what is the volume of the plasma?
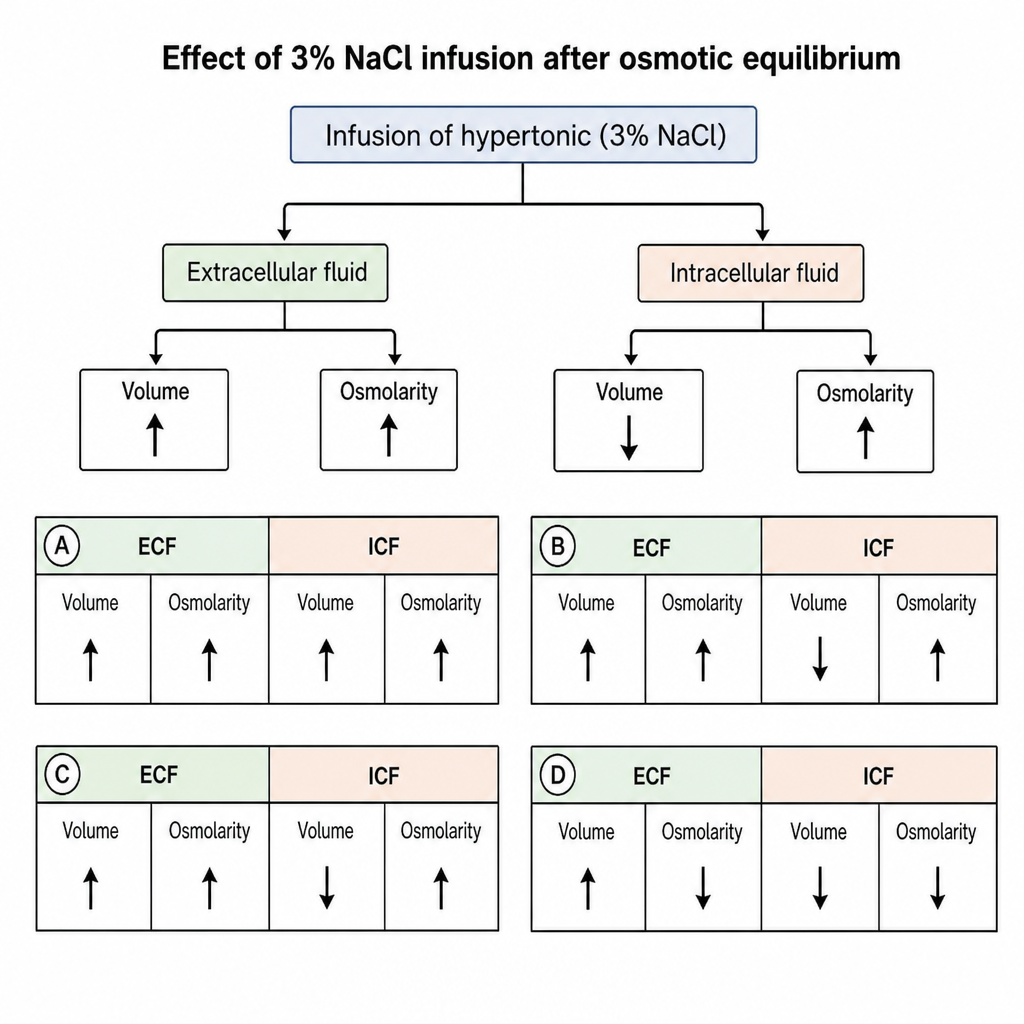
Which diagram represents the changes in extracellular and intracellular fluid volumes and osmolarities after the infusion of 3% NaCl, after osmotic equilibrium has been reached?
Calculate the osmolarity of a solution which contains 180 gm of glucose per dL, 117 gm of NaCl per dL, and 56 gm of BUN per dL.
Carpopedal spasm with normal serum ionic calcium level is due to:
Low calcium levels will cause which of the following?
The average value of total body water in a young man is what percentage of body weight?
Which of the following statements about shock is true?
Practice by Chapter
Body Fluid Compartments and Composition
Practice Questions
Osmolality and Tonicity
Practice Questions
Sodium and Water Balance
Practice Questions
Potassium Homeostasis
Practice Questions
Calcium and Phosphate Regulation
Practice Questions
Magnesium Metabolism
Practice Questions
Fluid Shifts Between Compartments
Practice Questions
Edema Formation Mechanisms
Practice Questions
Dehydration Physiology
Practice Questions
Disorders of Electrolyte Balance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app