
Bronchodilators — MCQs

Aminophylline inhibits which of the following enzymes?
The activation of muscarinic receptors in bronchiolar smooth muscle is associated with:
Which of the following is NOT a beta-2 agonist?
All of the following drugs are used for the treatment of urinary incontinence except:
Which of the following antimicrobials should not be given to a chronic asthmatic patient managed on theophylline therapy?
What is a contraindication of antimuscarinic drugs?
Maximum effect of bronchodilatation in asthma is caused by -
Tamsulosin belongs to
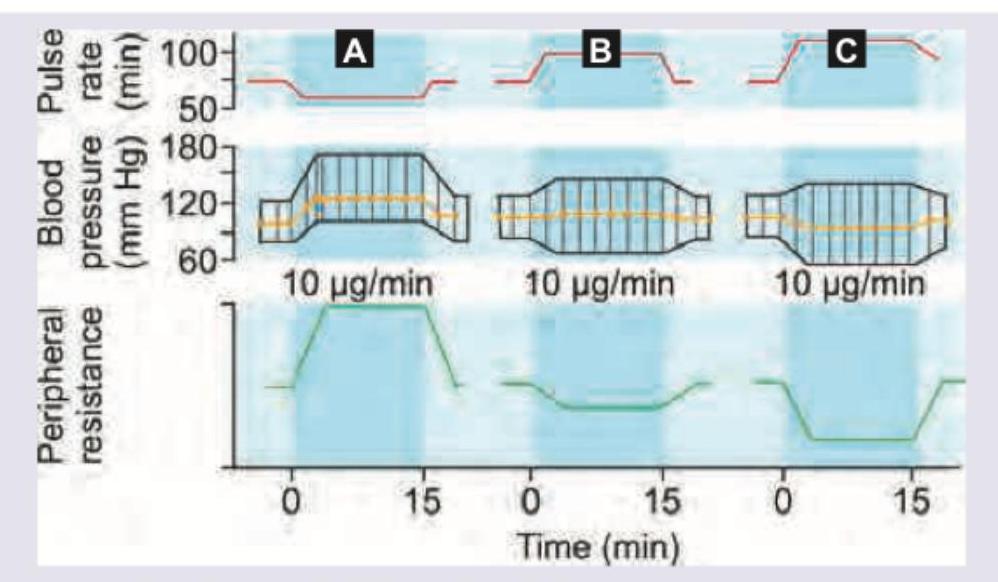
Which of the following statement is correct regarding the graph shown? (AllMS Nov 2016)
What is an atypical side effect of montelukast?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app