
Ethical Considerations in Pharmacogenomics — MCQs

DNA fingerprinting can be done with all, except:
Which of the following is not considered a pharmacogenetic condition?
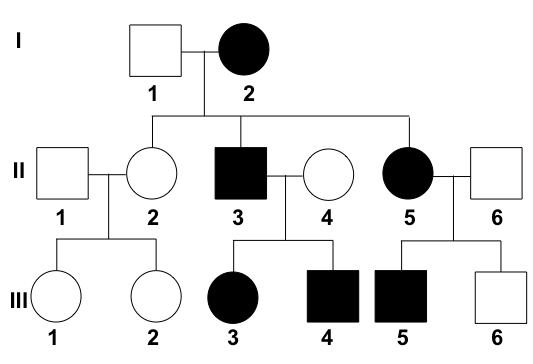
What is the interpretation of the given pedigree chart?
In the context of Indian regulations, what is the minimum number of Medical Termination of Pregnancy (MTP) cases a doctor must have performed to be eligible to perform an MTP?
Molecular genetic testing is used to detect all of the following except?
India is a country with different cultures and diverse languages. Which steps should a physician take to address the patient for better outcomes? 1. Insist on good communication 2. Insist on communication only via an interpreter 3. Treat them regardless of their cultural perceptions 4. The physician should consider the patient's religion and cultural perception Select the correct combination:
What is the primary health concern addressed by the Rashtriya Bal Swasthya Karyakram (RBSK)?
Which HLA gene is associated with abacavir hypersensitivity?
Which of the following does not cause hemolysis in G6PD deficiency?
All of the following drugs cause hemolysis in G-6PD deficiency except?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app