
Pediatric and Geriatric Pharmacology — MCQs

On this page
Which drug can be safely used in lactating mothers?
What is the minimum dose of tetracycline that causes discoloration of teeth?
What is the most dangerous effect of belladonna in very young children?
Which drug is implicated for prolonging the QT interval in a premature baby?
A premature infant is born with a patent ductus arteriosus. Its closure can be stimulated by administration of:
All of the following are reasons for reducing drug dosage in the elderly, EXCEPT:
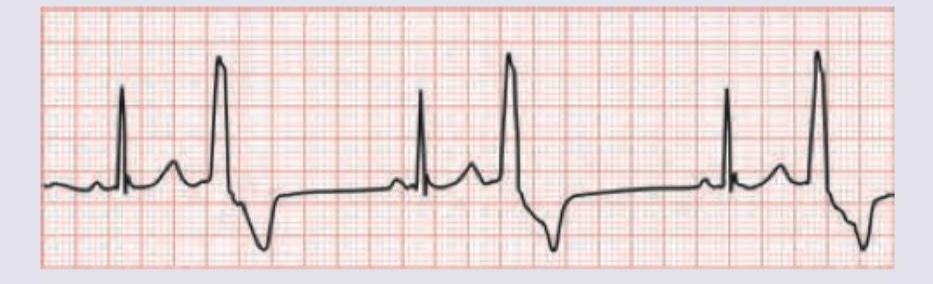
A 1-year-old child with moderate VSD is scheduled for surgery next month. For control of symptoms of CHF, a drug $X$ was given. The uneducated parents gave double the dose of drug resulting in the child developing listlessness and poor feeding. Based on the ECG shown, what is the drug prescribed and its side effect?
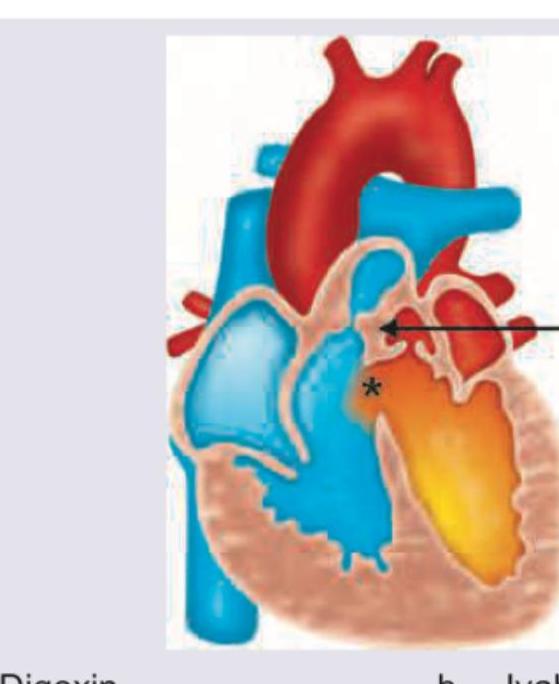
A neonate presents with a congenital heart disease as shown below. Which drug should be started immediately? (Recent NEET Pattern 2016-17)
A 3-year-old child presents with febrile seizures. All of the following are correct about rectal administration of diazepam except:

Which of the following statements are correct about oral rotavirus vaccines? I. The storage should be at 2-8°C II. The vaccine should be used within 2 hours of reconstitution or opening III. Past history of intussusception is a contraindication IV. The vaccine can be given if the baby has ongoing diarrhoea Select the answer using the code given below :
Practice by Chapter
Developmental Pharmacology
Practice Questions
Pediatric Dosing Principles
Practice Questions
Neonatal Pharmacology
Practice Questions
Pharmacotherapy in Children
Practice Questions
Age-Related Changes in Pharmacokinetics
Practice Questions
Age-Related Changes in Pharmacodynamics
Practice Questions
Polypharmacy in the Elderly
Practice Questions
Medication Adherence in Elderly
Practice Questions
Inappropriate Prescribing in Elderly
Practice Questions
Deprescribing Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app