
General Pharmacology — MCQs

On this page
Which of the following is a prodrug?
Which of the following is an immunostimulant?
Which of the following statements is wrong?
Liposomes are used for drug delivery in all of the following except?
Effects mediated by H1 histamine receptor include?
Monitoring of drug level is not required with which of the following medications?
Which of the following are NOT typically administered intradermally?
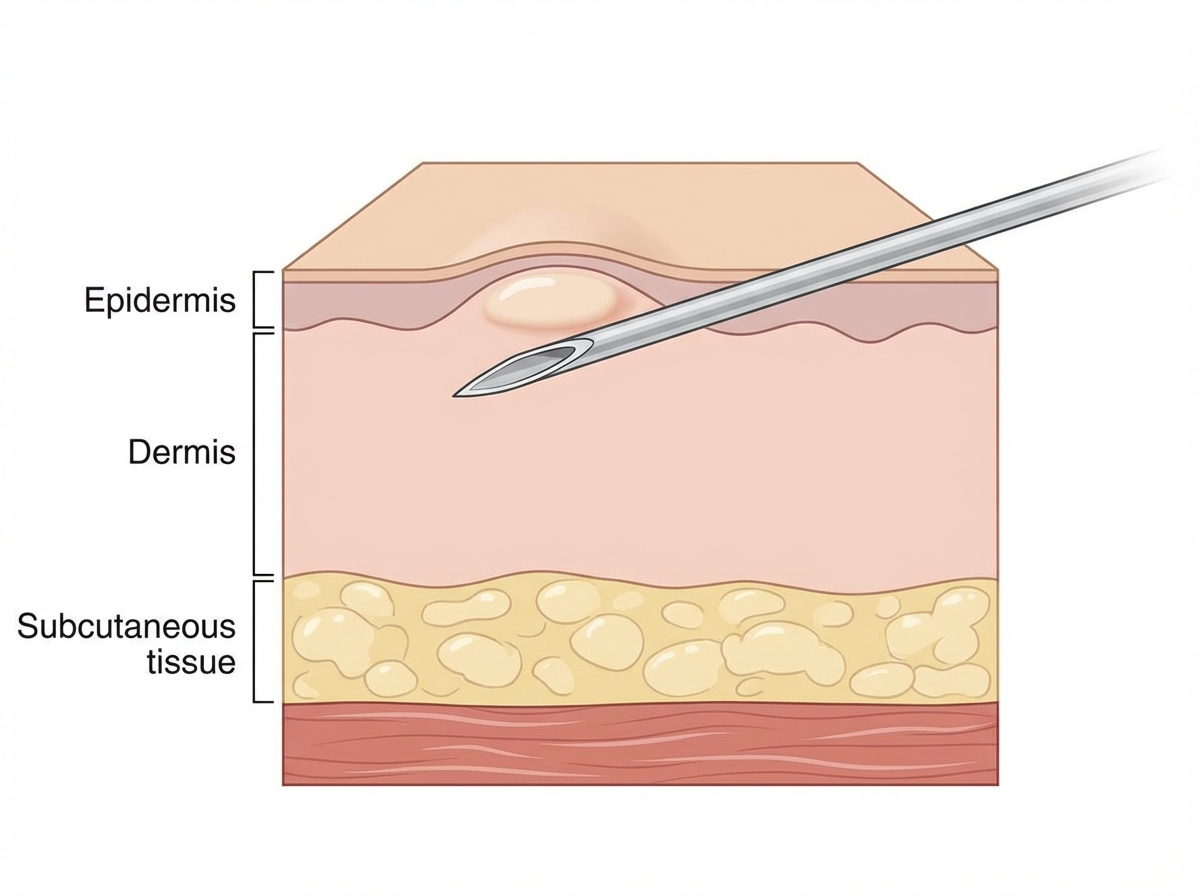
Which of the following routes of administration is shown in the given diagram?
Therapeutic drug monitoring is indicated for which of the following drugs?
Which of the following actions is not caused by H1 receptor?
Practice by Chapter
Pharmacokinetics: Absorption and Distribution
Practice Questions
Pharmacokinetics: Metabolism and Excretion
Practice Questions
Pharmacodynamics and Receptor Theory
Practice Questions
Drug-Receptor Interactions and Dose-Response
Practice Questions
Pharmacogenetics and Personalized Medicine
Practice Questions
Adverse Drug Reactions and Toxicity
Practice Questions
Drug Interactions
Practice Questions
Drug Development and Regulation
Practice Questions
Pediatric and Geriatric Pharmacology
Practice Questions
Placental Transfer and Lactation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app