
General Pharmacology — MCQs

On this page
All of the following can cause histamine release except?
What is acute or rapidly developing tolerance to a drug?
Which of the following drugs has a narrow therapeutic index?
A widely used drug that suppresses cellular immunity, inhibits prostaglandin and leukotriene synthesis, and increases the catabolism of IgG antibody is:
Most essential medicines should be formulated as which of the following?
Which drug possesses antagonistic action at histamine, serotonin, and muscarinic receptors?
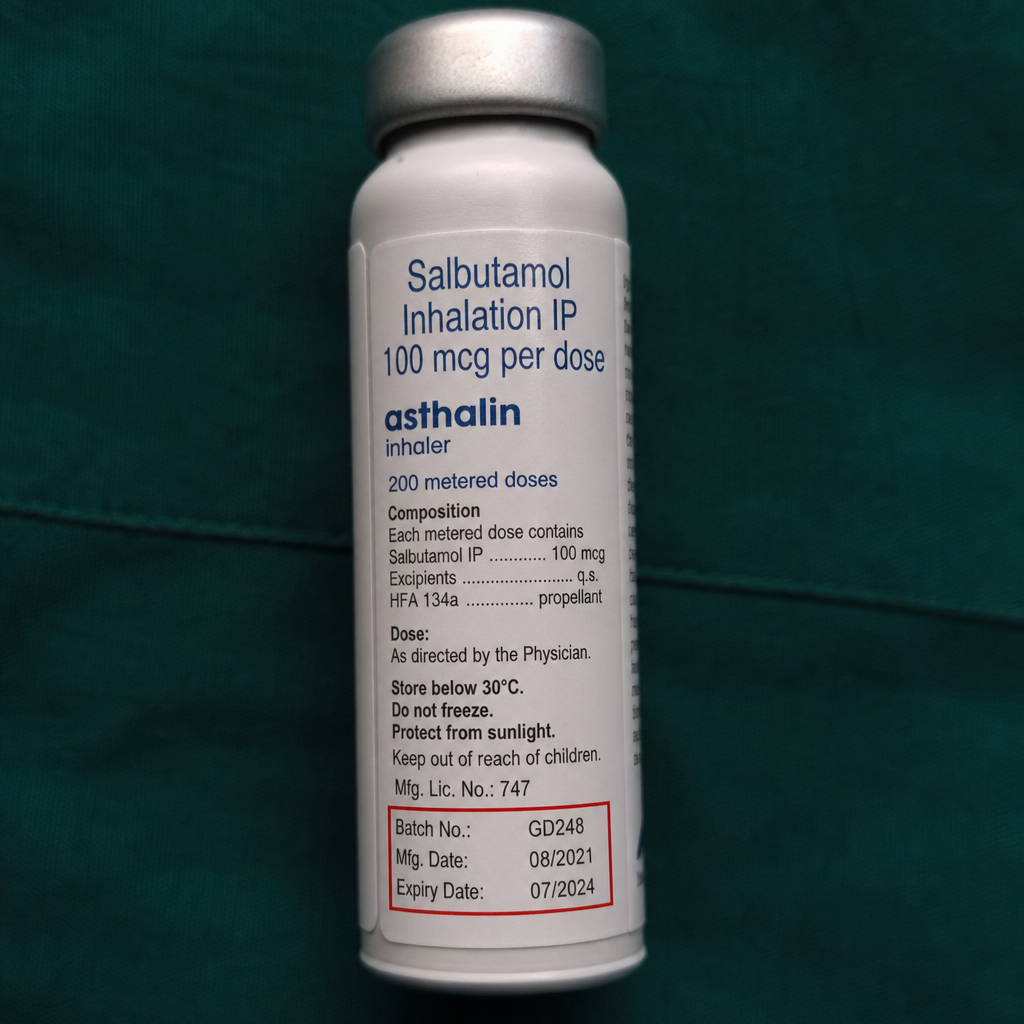
What is the shelf life of salbutamol in this preparation?
A farmer presented in the OPD clinic with sweating, lacrimation, and pinpoint pupils. What type of poisoning is suspected?
What is the typical sequence of clinical trials for a new drug?
All the following regarding prostaglandin analogues are true except?
Practice by Chapter
Pharmacokinetics: Absorption and Distribution
Practice Questions
Pharmacokinetics: Metabolism and Excretion
Practice Questions
Pharmacodynamics and Receptor Theory
Practice Questions
Drug-Receptor Interactions and Dose-Response
Practice Questions
Pharmacogenetics and Personalized Medicine
Practice Questions
Adverse Drug Reactions and Toxicity
Practice Questions
Drug Interactions
Practice Questions
Drug Development and Regulation
Practice Questions
Pediatric and Geriatric Pharmacology
Practice Questions
Placental Transfer and Lactation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app