
Endocrine Pharmacology — MCQs

On this page
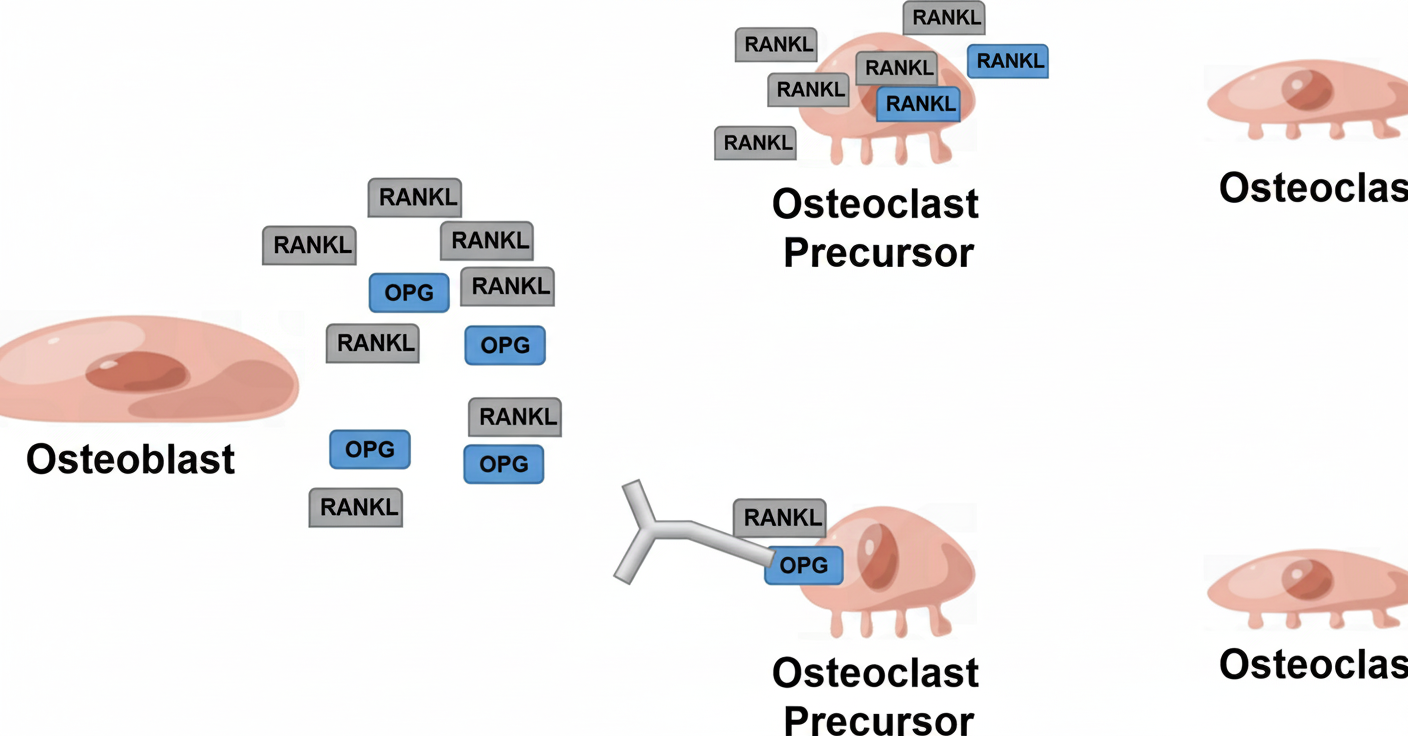
A drug used in the management of osteoporosis has the mechanism of action depicted in the accompanying figure. What is the likely identity of this drug?
Metformin is NOT effective in lowering of blood sugar level in which of the following patients?
Which of the following does not cause insulin release?
A 29-year-old male patient presents to the OPD with a 10-year history of coarse facial features and progressive enlargement of the hands and feet. Laboratory evaluation revealed elevated IGF-1 and non-suppressible growth hormone levels after the 75 g glucose challenge test. A diagnosis of acromegaly is made. Which of the following drugs is preferred for the management of this patient?
A 55-year-old diabetic patient on metformin develops lactic acidosis after a contrast-enhanced CT scan. What is the mechanism by which metformin contributed to this complication?
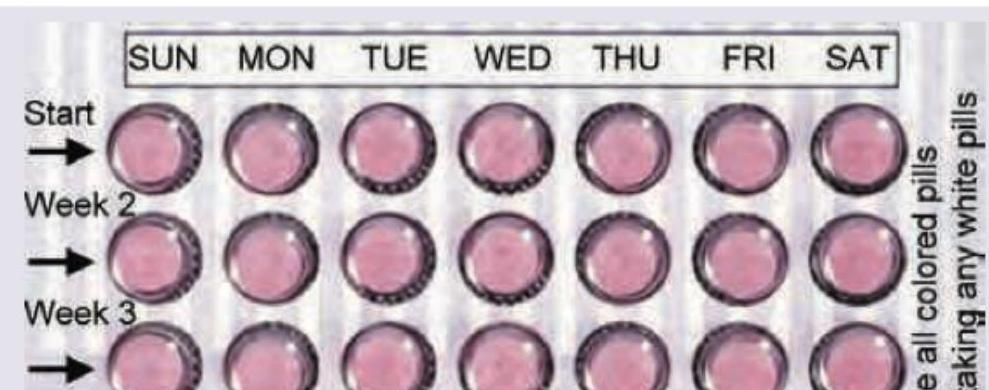
A 28-year-old woman is prescribed an oral contraceptive pill. The packaging shown in the image contains pills organized by weeks with all pills being the same color. What type of combined oral contraceptive preparation is this?
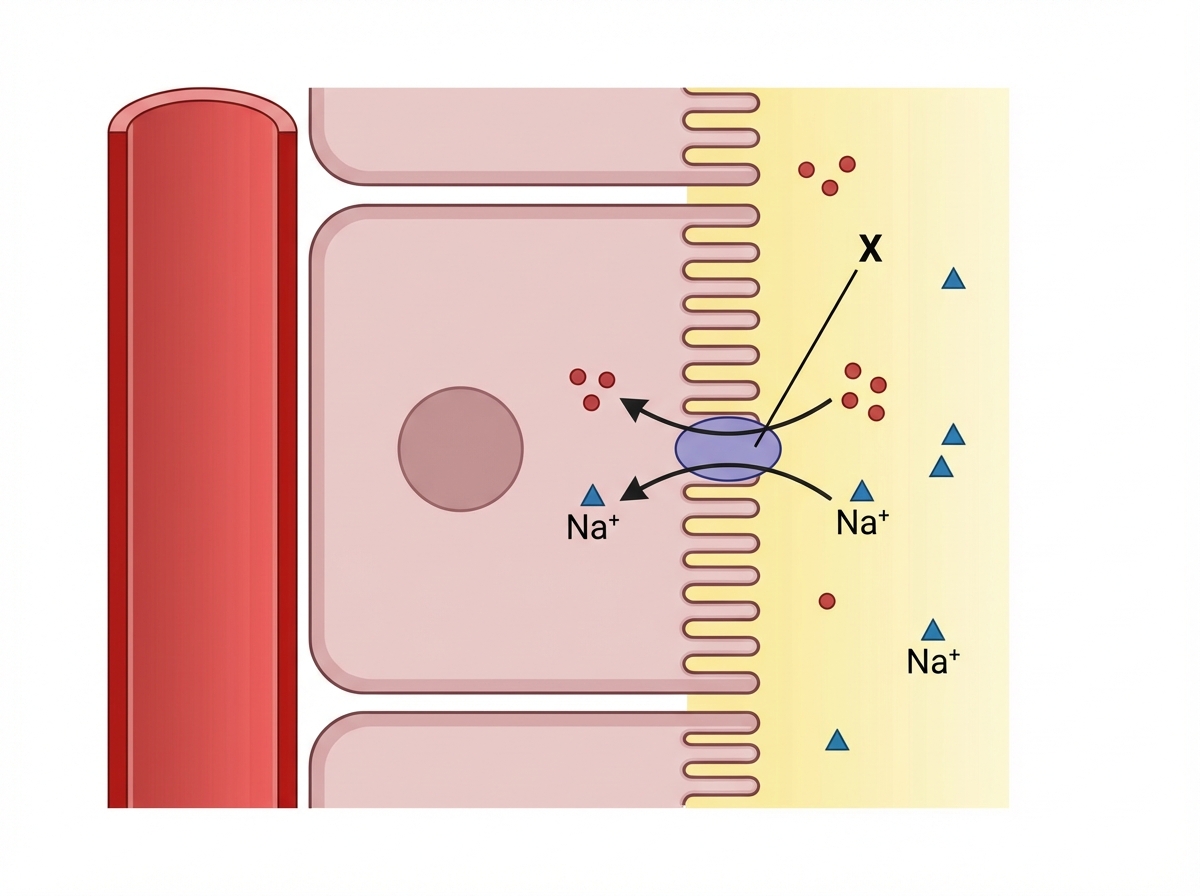
Which of the following drugs will act on X to inhibit sugar absorption from the PCT of kidney?
A 60-year-old post-menopausal woman presents with low back ache and pain in all legs muscles. Her lab reports show normal serum calcium, phosphate and normal serum alkaline phosphatase. For management of this condition, which of the following drugs is given by intranasal route?
A primigravida at 38 weeks pregnancy was put on oxytocin drip in view of slow labour at the rate of 30 mIU/min by the newly appointed registrar. She complains of confusion and starts throwing fits. What electrolyte imbalance is expected to have happened in this case?
Which one of the following is correct regarding arginine vasopressin antagonist Tolvaptan?
Practice by Chapter
Hypothalamic and Pituitary Hormones
Practice Questions
Thyroid Drugs and Antithyroid Agents
Practice Questions
Insulin and Oral Hypoglycemic Agents
Practice Questions
Adrenocorticosteroids
Practice Questions
Sex Hormones: Estrogens and Progestins
Practice Questions
Androgens and Anabolic Steroids
Practice Questions
Hormonal Contraceptives
Practice Questions
Drugs Affecting Calcium Metabolism
Practice Questions
Drugs for Osteoporosis
Practice Questions
Pharmacological Management of Obesity
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app