
Endocrine Pharmacology — MCQs

On this page
Magnesium is used in the treatment of which of the following conditions?
What is the standard dosage of Testosterone?
Continuous administration of GnRH -
What is a common side effect of clomiphene citrate?
All of the following drugs cause osteoporosis except?
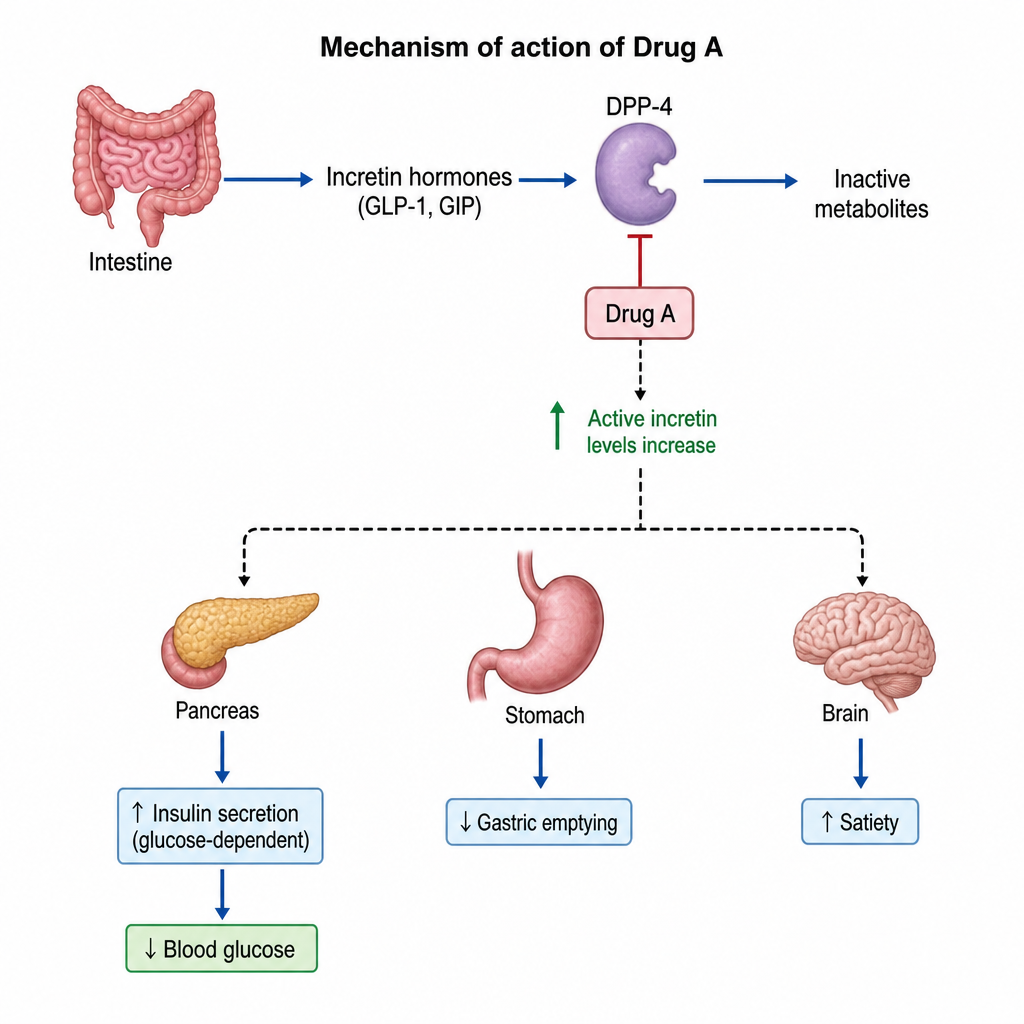
Based on the given mechanism of action as shown in the Figure, Drug A is likely to be:
Danazol is used in all of the following conditions except:
An elderly male has benign prostatic hyperplasia. Which of the following medications can be used to suppress prostatic growth?
Gestrinone has the following actions except?
All of the following are effects of estrogen, EXCEPT:
Practice by Chapter
Hypothalamic and Pituitary Hormones
Practice Questions
Thyroid Drugs and Antithyroid Agents
Practice Questions
Insulin and Oral Hypoglycemic Agents
Practice Questions
Adrenocorticosteroids
Practice Questions
Sex Hormones: Estrogens and Progestins
Practice Questions
Androgens and Anabolic Steroids
Practice Questions
Hormonal Contraceptives
Practice Questions
Drugs Affecting Calcium Metabolism
Practice Questions
Drugs for Osteoporosis
Practice Questions
Pharmacological Management of Obesity
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app