
Drugs in Cardiac Arrest — MCQs

Which one of the following was traditionally considered the drug of choice for ventricular tachycardia in myocardial infarction?
Patient with pulmonary fibrosis. Which antiarrhythmic drug is contraindicated?
Which of these is least effective as first-line treatment for dangerous hyperkalemia?
Which of the following rhythms associated with cardiac arrest is considered shockable?
Which drug is used as an adjunct to epinephrine in refractory ventricular fibrillation/ventricular tachycardia during cardiac arrest?
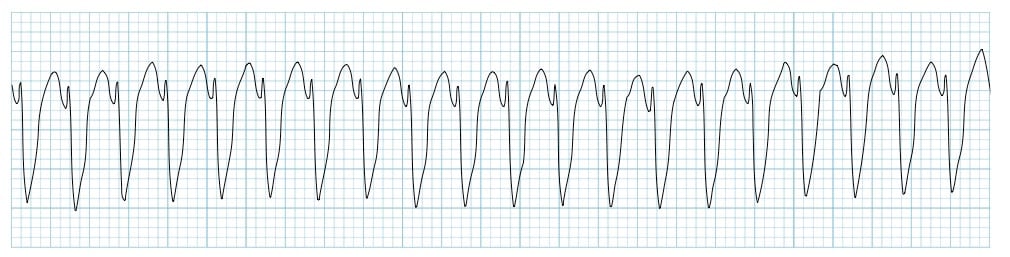
A patient is pulseless with the following rhythm shown in the ECG. What is the next best step in management?
As per the recent guidelines of resuscitation, what should be done if asystole is not responding to two consecutive doses of epinephrine?
Which local anesthetic is considered the most cardiotoxic?
In ACLS, which antiarrhythmic drug can be given following ventricular fibrillation after cardiac arrest other than epinephrine?
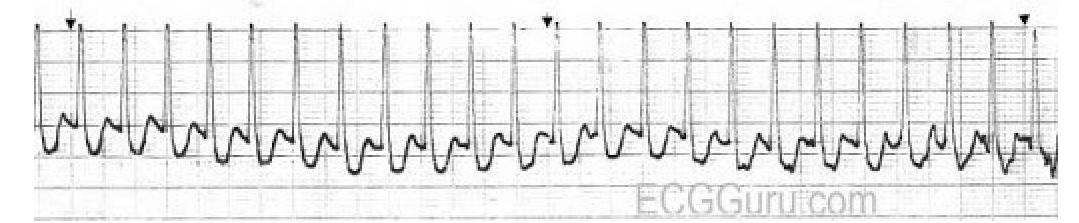
Identify the diagnosis based on the provided ECG image.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app