
Topical Corticosteroids — MCQs

Which of the following is a contraindication to topical steroids?
All of the following are topical steroids EXCEPT ?
Which of the following is not a side effect of topical beta blockers?
Which of the following statements about Ciclesonide is incorrect?
What is the primary mechanism by which steroids exert their anti-inflammatory action?
Hydrocortisone Acetate is injected in a painful arthritic TMJ to?
Anti-inflammatory action of steroids is due to
Dapsone is NOT used in:
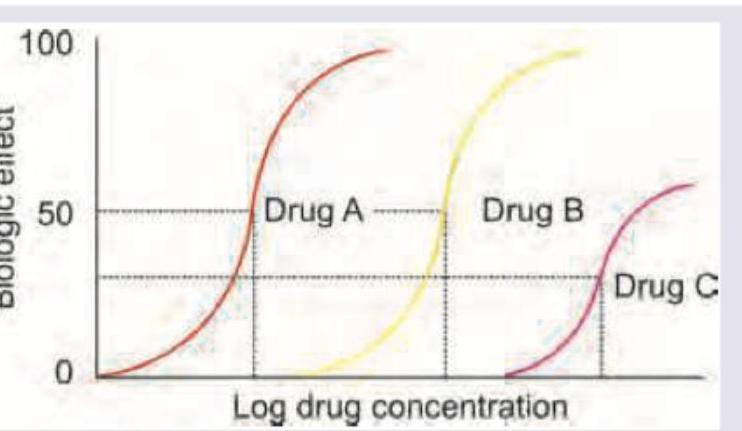
Which of the following statement is correct regarding the given DRC? (AllMS Nov 2016)
Which of the following is an example of topical administration producing only local effects (not systemic)?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app