
Drugs for Gastrointestinal Diseases — MCQs

On this page
Which of the following anticholinergic agents is used for the treatment of peptic ulcer disease?
All of the following are true about Ondansetron except?
All of the following are true about Nizatidine except?
Which laxative acts by opening of Chloride channels?
Which drug is used in cancer chemotherapy-induced vomiting?
Magaldrate is converted by gastric acid to which of the following?
Which of the following is a correct triple drug regimen for the treatment of Helicobacter pylori infection?
Which drug is most appropriate for treating diarrhea in a patient treated for colorectal carcinoma with 5-fluorouracil?
A patient presents with GERD. Which drug helps in contraction of LES and increases gastric emptying?
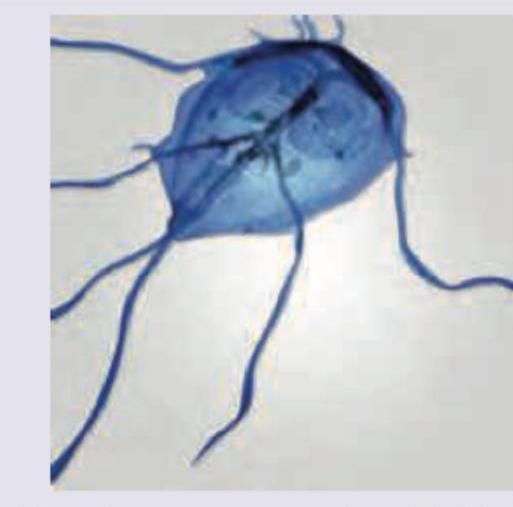
All are used in treatment for the GIT parasite shown below except:
Practice by Chapter
Acid-Peptic Disease Therapeutics
Practice Questions
Proton Pump Inhibitors
Practice Questions
H2 Receptor Antagonists
Practice Questions
Antacids and Mucosal Protectants
Practice Questions
Antiemetics
Practice Questions
Prokinetic Agents
Practice Questions
Laxatives and Purging Agents
Practice Questions
Antidiarrheal Drugs
Practice Questions
Drugs for Inflammatory Bowel Disease
Practice Questions
Pancreatic Enzyme Supplements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app