
Drugs for Gastrointestinal Diseases — MCQs

On this page
Which of the following drugs is NOT used in the management of obesity?
What is the drug of choice for the medical management of bleeding esophageal varices?
Which drug is NOT used in the treatment of H. pylori infection?
What is true regarding sulfasalazine?
Levosulpiride acts as an antagonist of which central dopamine receptor?
Teduglutide is used in small bowel syndrome because its action is similar to which of the following?
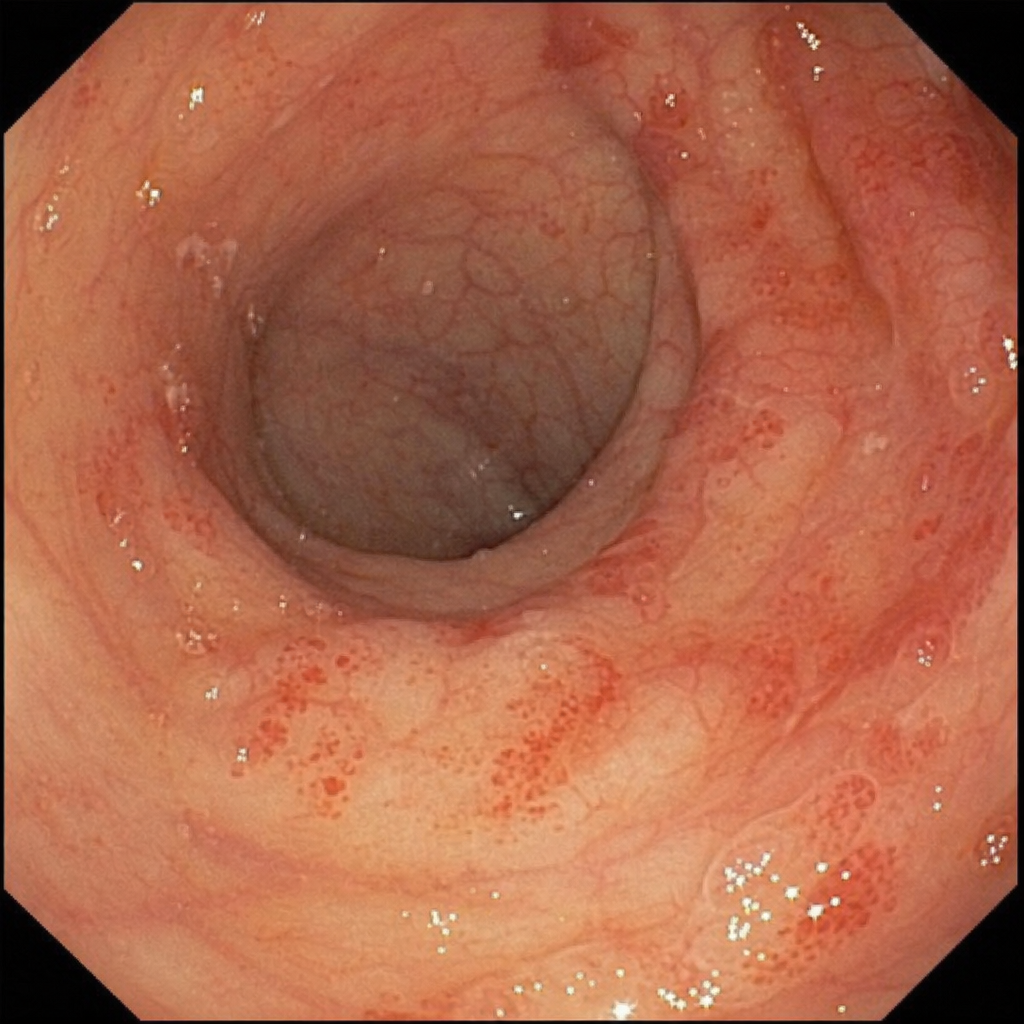
The following adverse drug reaction seen in colonoscopy view is due to which of the following agents?
Which of the following drugs does NOT cause peptic ulcers?
Gynaecomastia may be associated with the administration of which drug?
Indicate the drug which does not improve lower esophageal sphincter tone or prevent gastroesophageal reflux, but is used as the first-line treatment of gastroesophageal reflux disease?
Practice by Chapter
Acid-Peptic Disease Therapeutics
Practice Questions
Proton Pump Inhibitors
Practice Questions
H2 Receptor Antagonists
Practice Questions
Antacids and Mucosal Protectants
Practice Questions
Antiemetics
Practice Questions
Prokinetic Agents
Practice Questions
Laxatives and Purging Agents
Practice Questions
Antidiarrheal Drugs
Practice Questions
Drugs for Inflammatory Bowel Disease
Practice Questions
Pancreatic Enzyme Supplements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app