
Drugs for Gastrointestinal Diseases — MCQs

On this page
A patient on cisplatin therapy develops intractable vomiting on the third day of treatment. What is the agent of choice for controlling this vomiting?
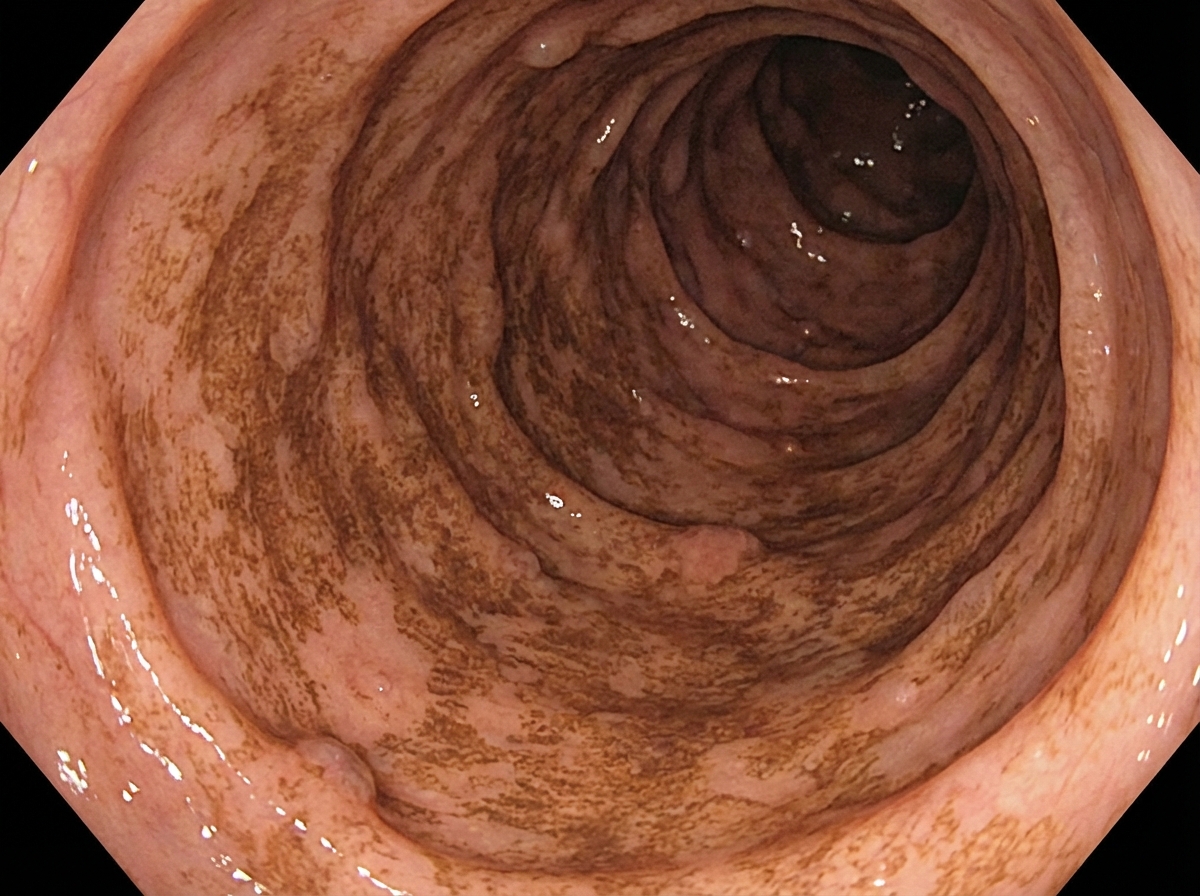
Which of the following drugs causes the observed effect on colonoscopic view?
Why is atropine added to commercial preparations containing diphenoxylate?
Which of the following is NOT a gastrointestinal effect of metoclopramide?
What is the most common side effect of the 5-HT3 antagonist drug alosetron?
The inhibition of hydrochloric acid (HCl) secretion by omeprazole occurs within an hour, reaches a peak at 2 hours, and plateaus by the 4th day. After how many days will the secretion gradually normalize?
Certolizumab is used in the treatment of:
Which of the following drugs is used in the management of drug-induced ulcers?
Which of the following is the drug of choice for the treatment of peptic ulcer disease?
Which laxative is used in the management of hepatic encephalopathy?
Practice by Chapter
Acid-Peptic Disease Therapeutics
Practice Questions
Proton Pump Inhibitors
Practice Questions
H2 Receptor Antagonists
Practice Questions
Antacids and Mucosal Protectants
Practice Questions
Antiemetics
Practice Questions
Prokinetic Agents
Practice Questions
Laxatives and Purging Agents
Practice Questions
Antidiarrheal Drugs
Practice Questions
Drugs for Inflammatory Bowel Disease
Practice Questions
Pancreatic Enzyme Supplements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app