
Drug Interactions — MCQs

On this page
Cimetidine inhibits the metabolism of all of the following drugs except?
Which of the following drugs can cause a disulfiram-like reaction?
A patient with rheumatoid arthritis is taking indomethacin and an ACE inhibitor for hypertension. What potential side effect is likely to be seen?
Carbamazepine and erythromycin were given to a patient, and he presented with ataxia and dizziness. Which of the following is the reason for the symptoms?
Imipramine and Diphenhydramine are given together to a patient. Why is this combination considered irrational?
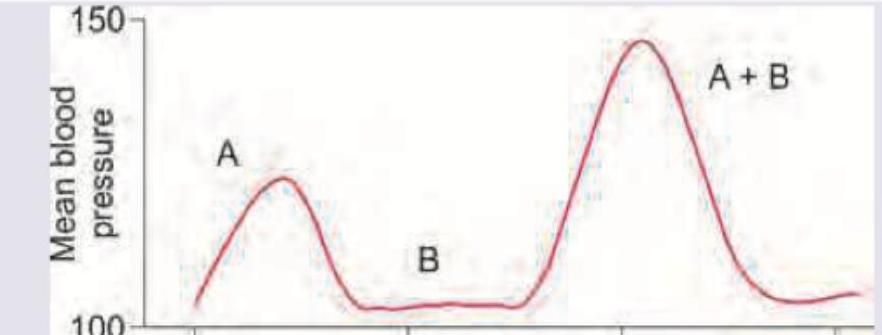
Drug A is epinephrine and drug B is cocaine. The effect of both drugs given together on the blood pressure of a patient was evaluated in comparison with effect of individual drugs on BP. The following curve represents:
A 25-year-old newly married female on liver enzyme inducers is requesting contraceptive advice in family planning clinic. Which of the following would be the most reliable method of contraception for her?
The drugs which may interfere with the efficacy of oral contraceptives and increase the failure rates are all of the following EXCEPT
Which one of the following drugs does NOT interfere with efficacy of oral contraceptive pills and increase the failure rates?
A patient is on phenytoin for a seizure disorder. He was prescribed sucralfate 4 times a day for peptic ulcers. What should be the minimum duration of time between consumption of these drugs?
Practice by Chapter
Mechanisms of Drug Interactions
Practice Questions
Pharmacokinetic Interactions
Practice Questions
Pharmacodynamic Interactions
Practice Questions
Drug-Food Interactions
Practice Questions
Drug-Disease Interactions
Practice Questions
Clinically Significant Drug Interactions
Practice Questions
Computer Systems for Detecting Drug Interactions
Practice Questions
Management of Drug Interactions
Practice Questions
Drug Interactions in Special Populations
Practice Questions
Role of P-glycoprotein in Drug Interactions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app