
Diuretics — MCQs

On this page
Gitelman's syndrome resembles the effects of which of the following drugs?
What is the most clinically significant electrolyte disturbance caused by loop diuretics?
Mannitol is most commonly used for which of the following conditions?
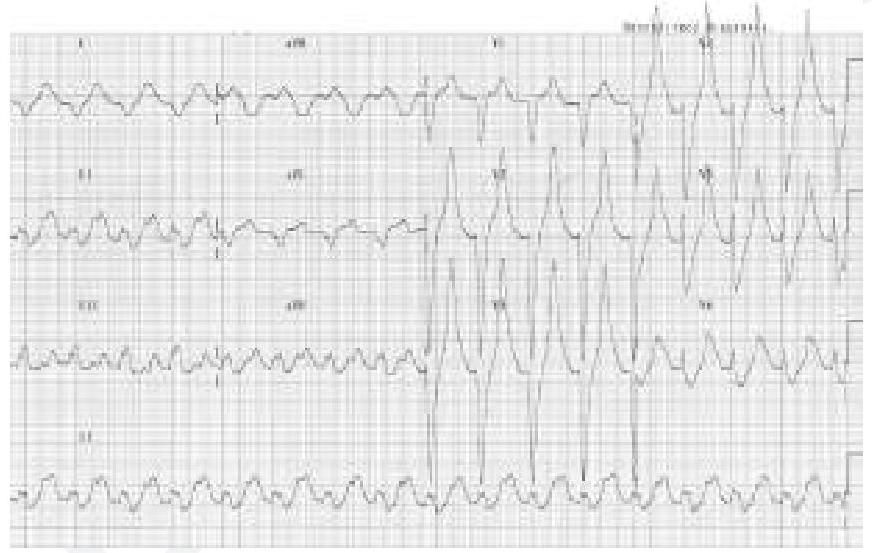
A patient who is a known case of hypertension on multiple anti-hypertensive medications came to OPD. His ECG finding is given below. Which of the following drugs is responsible for the ECG finding? (Image of ECG finding)
Theophylline by what mechanism causes diuresis?
Which of the following is not a side effect of thiazide diuretics?
Which diuretic is most likely to cause hyponatremia by impairing free water excretion?
How do thiazides cause hypercalcemia?
Which diuretic is known to cause the maximum potassium loss?
Which diuretic inhibits the Na+-K+-2Cl- symporter in the thick ascending limb of the loop of Henle?
Practice by Chapter
Carbonic Anhydrase Inhibitors
Practice Questions
Loop Diuretics
Practice Questions
Thiazide and Thiazide-Like Diuretics
Practice Questions
Potassium-Sparing Diuretics
Practice Questions
Carbonic Anhydrase Inhibitors
Practice Questions
Osmotic Diuretics
Practice Questions
Combination Diuretic Therapy
Practice Questions
Diuretics in Heart Failure
Practice Questions
Diuretics in Hypertension
Practice Questions
Diuretics in Renal Disorders
Practice Questions
Adverse Effects and Drug Interactions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app