
Diuretics — MCQs

On this page
A group of people are travelling to the mountains, and a girl starts complaining of mountain sickness. What is the drug of choice?
A patient having hypertension is on thiazides and is complaining of fatigue and hypokalemia. Which of the following drugs can prevent potassium loss?
A 35-year-old male experiences headache, nausea, and shortness of breath while trekking. The physician prescribes a drug to alleviate his symptoms. The drug administered primarily acts on which part of the nephron?
Which of the following carbonic anhydrase inhibitors primarily acts on the part labeled 'D' in the given diagram of a nephron?
A 50-year-old woman was prescribed a diuretic by a doctor to manage hypertension. Which of the following diuretics acts on site 'A' as marked in the given image?
A patient on hydrochlorothiazide develops renal stones. What explains this adverse effect?
By what primary mechanism does hydrochlorothiazide help prevent the formation of calcium stones?
A patient is started on hydrochlorothiazide for hypertension and later develops renal stones. Which metabolic effect of hydrochlorothiazide is most likely responsible?
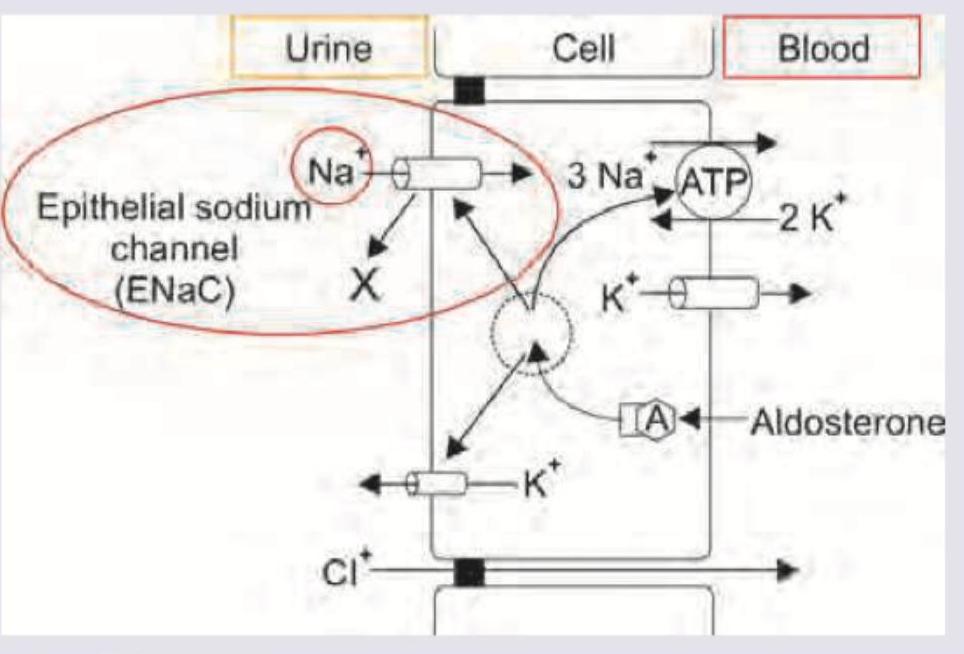
The image shows drug 'X' blocking a channel in the renal tubule. Which of the following drugs is 'X'?
A 66-year-old male presents to the outpatient cardiology clinic for evaluation of suspected primary hypertension. His blood pressure is elevated to 169/96 mm Hg, and his heart rate is 85/min. Physical examination reveals an overweight male with regular heart and lung sounds. Following repeated elevated blood pressure measurements, the diagnosis is made and the patient is started on hydrochlorothiazide. Of the following options, which is a side effect that one could experience from thiazide-like diuretics?
Practice by Chapter
Carbonic Anhydrase Inhibitors
Practice Questions
Loop Diuretics
Practice Questions
Thiazide and Thiazide-Like Diuretics
Practice Questions
Potassium-Sparing Diuretics
Practice Questions
Carbonic Anhydrase Inhibitors
Practice Questions
Osmotic Diuretics
Practice Questions
Combination Diuretic Therapy
Practice Questions
Diuretics in Heart Failure
Practice Questions
Diuretics in Hypertension
Practice Questions
Diuretics in Renal Disorders
Practice Questions
Adverse Effects and Drug Interactions
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app