
Carbonic Anhydrase Inhibitors — MCQs

Renal stones are seen as a complication by using the following drug:
Which of the following is an example of topical administration producing only local effects (not systemic)?
Which of the following antidiabetic drugs (other than insulin) is indicated as adjunct therapy for the management of both type I and type II diabetes mellitus?
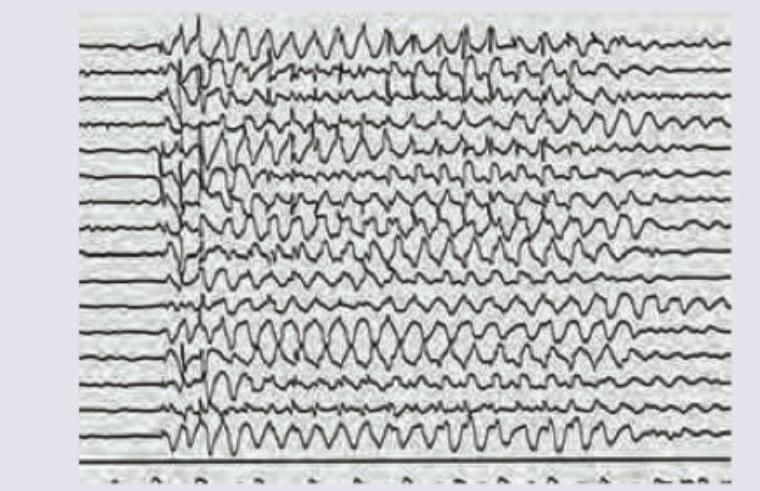
A 6-year-old child has poor school performance. On scolding by teacher abnormal behavior is noted. EEG is performed. Which of the following drugs will cause worsening of the patient?
A young male, Farhan, suffers from a seizure disorder which is characterized by tonic rigidity of limbs followed in 20-30 seconds by tremors progressing to massive jerking of the body. This clonic phase lasts for 1-3 minutes. The anti-seizure drug of choice for this patient is:
A patient presents with painful oral ulcers and target lesions on extremities. Which drug is MOST likely to cause this condition?
Furosemide causes all except -
How do thiazides cause hypercalcemia?
Furosemide -induced hearing loss occurs primarily by damaging which structure?
A 26-year-old man diagnosed with diabetes insipidus was started on hydrochlorothiazide. The beneficial effect of hydrochlorothiazide in this patient is due to which of the following mechanisms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app