
Clinical Pharmacology and Drug Toxicity — MCQs

On this page
Toxic shock syndrome occurs after one of the following vaccinations :
Misoprostol can be used in obstetric practice by the following routes except:
Which of the following local anaesthetics causes irreversible cardiac arrest if it is given intravenously ?
Which one of the following is an absolute contraindication for administration of killed vaccine?
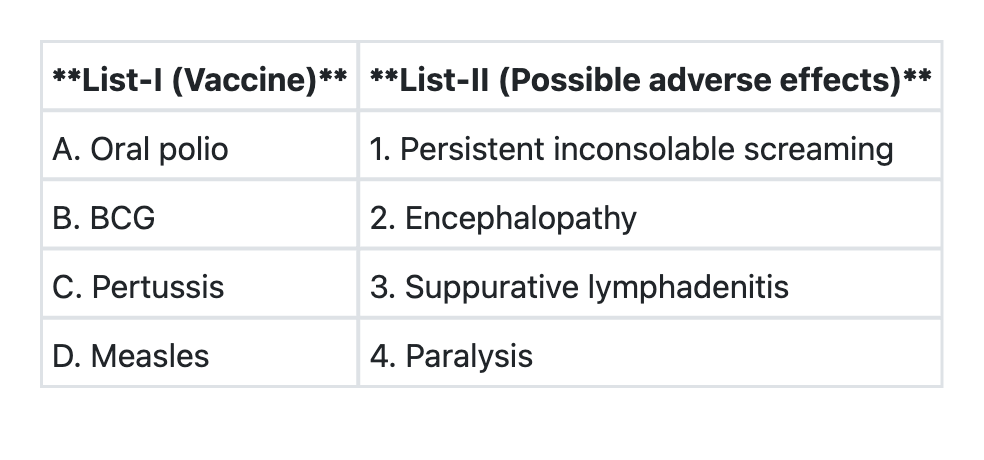
Match List-I with List-II and select the correct answer using the code given below the Lists:
Intramuscular injection of iron dextran is given by ‘Z’ technique to:
Absolute contraindication to combined oral contraceptive is:
Which of the following drugs should be avoided in the first-line ART regimens because of its well recognized metabolic toxicities ?
Which of the following statements regarding the composition of common crystalloid solutions is correct ?
Absolute contraindication for the use of OCPs is:
Practice by Chapter
Principles of Clinical Pharmacology
Practice Questions
Therapeutic Drug Monitoring
Practice Questions
Drug Toxicity and Overdose
Practice Questions
Antidotes and Their Applications
Practice Questions
Management of Drug Poisoning
Practice Questions
Drug-Induced Liver Injury
Practice Questions
Drug-Induced Kidney Injury
Practice Questions
Drug-Induced Blood Dyscrasias
Practice Questions
Drug-Induced QT Prolongation
Practice Questions
Pharmacovigilance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app