
Clinical Pharmacology and Drug Toxicity — MCQs

On this page
Absolute contraindication to combined oral contraceptive is:
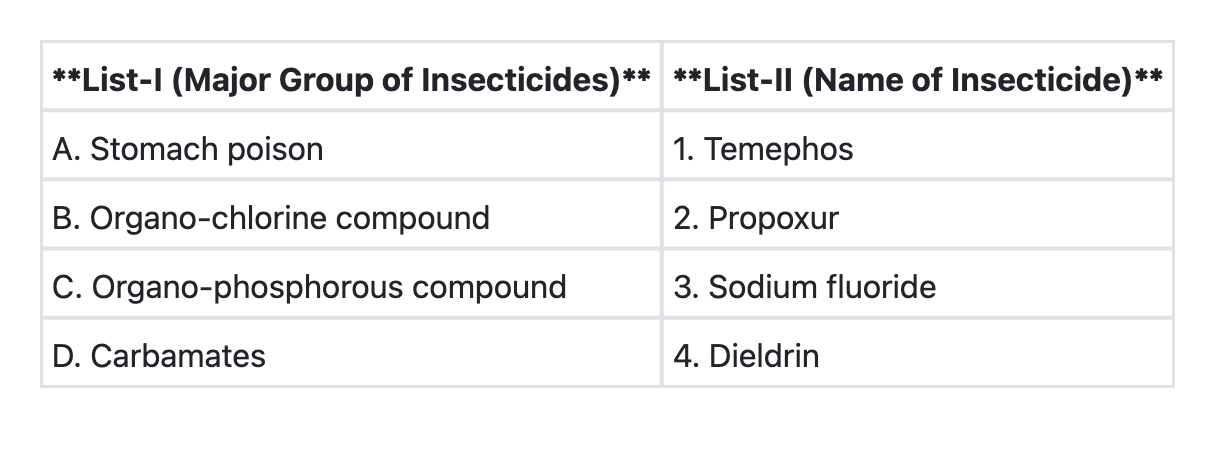
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which one of the following antihypertensive drugs is NOT safe during pregnancy?
A patient has been diagnosed with Primary Open Angle Glaucoma (POAG). On eliciting history, it is observed that the patient is a known case of bronchial asthma. What is the drug of choice for POAG in this patient?
A man was brought to the emergency room after poisoning with an unknown substance. Muscarinic poisoning was suspected and he was treated for the same. What is the possible presenting feature which led to the diagnosis?
Match the following drugs in Column A with their contraindications in Column B. | Column A | Column B | | :-- | :-- | | 1. Morphine | 1. QT prolongation | | 2. Amiodarone | 2. Thromboembolism | | 3. Vigabatrin | 3. Pregnancy | | 4. Estrogen preparations | 4. Head injury |
A patient presented with dizziness, cool clammy skin, pinpoint pupil with blue lips and fingernails suffering from respiratory depression. The patient was producing a pink frothy sputum on coughing. The drug used to reverse the effects is?
A child went to temple along with his grandmother. He developed altered sensorium, BP of $150 / 90 \mathrm{~mm} \mathrm{Hg}$, sweating, palpitations, priapism, and mouth secretion all at once. What drug can be given to this patient?
A female was given morphine sulphate during labour for pain but she developed respiratory distress. Which of the following will be the correct antidote?
A kid went to a temple with his grandmother and was constantly crying. On examination he had excruciating pain, hypertension, increased heart rate, sweating profusely, priapism and cold clammy skin. What should be the treatment given to the patient?
Practice by Chapter
Principles of Clinical Pharmacology
Practice Questions
Therapeutic Drug Monitoring
Practice Questions
Drug Toxicity and Overdose
Practice Questions
Antidotes and Their Applications
Practice Questions
Management of Drug Poisoning
Practice Questions
Drug-Induced Liver Injury
Practice Questions
Drug-Induced Kidney Injury
Practice Questions
Drug-Induced Blood Dyscrasias
Practice Questions
Drug-Induced QT Prolongation
Practice Questions
Pharmacovigilance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app