
Clinical Pharmacology and Drug Toxicity — MCQs

On this page
A patient came to the hospital with muscle weakness, diarrhea, and bradycardia. He was diagnosed with organophosphate poisoning for which atropine was administered. After atropine administration, which of the following changes are not seen?
A 25-year-old woman presents to the emergency department 6 hours after ingesting a large quantity of paracetamol tablets. What is the most likely progression of paracetamol poisoning in this case?
A 50-year-old factory worker was brought to the emergency room with complaints of headache, vomiting, and blurring of vision after he consumed local spirit. Which of the following is used for the treatment of his condition?
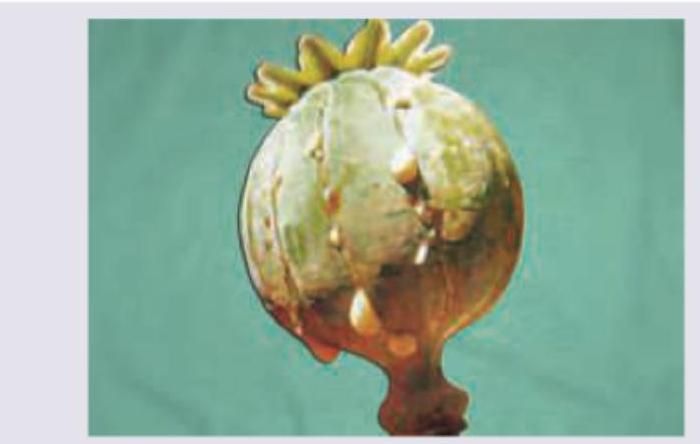
Which of the following is a non-narcotic active principle of the opium poppy shown in the image below?
The toxin shown below will cause:

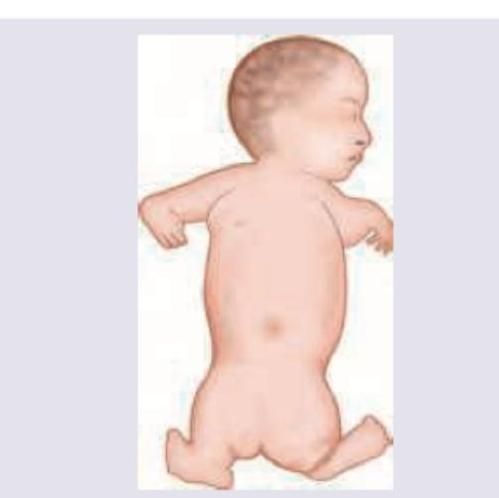
Which of the following drugs taken by the mother during pregnancy can cause the congenital defect shown in the image?

The condition shown in the image can be seen with all of the following EXCEPT:

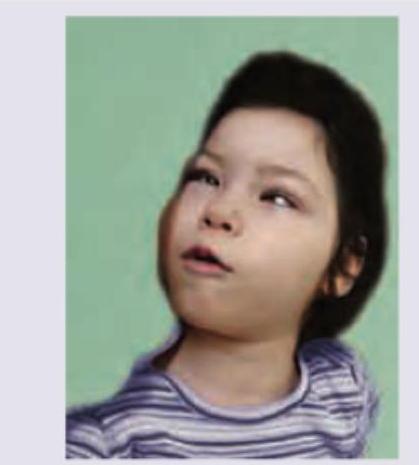
A 6-year-old child was having multiple vomiting episodes after eating at mid-day meal scheme in school. The Doctor at PHC gave injectable anti-emetics after which the child developed following posturing. What is the clinical diagnosis and what drug should be given to counteract this posturing?
A 35-year-old farmer consumed a pesticide due to inability to repay loans. On examination he is having increased sweating, salivation and muscle fasciculations. The family members have also brought the empty canister of insecticide. All are correct about the condition except: (Recent NEET Pattem 2016-17)
The following malformation in a baby due to drug intake by mother is classified as \qquad ADR?
Practice by Chapter
Principles of Clinical Pharmacology
Practice Questions
Therapeutic Drug Monitoring
Practice Questions
Drug Toxicity and Overdose
Practice Questions
Antidotes and Their Applications
Practice Questions
Management of Drug Poisoning
Practice Questions
Drug-Induced Liver Injury
Practice Questions
Drug-Induced Kidney Injury
Practice Questions
Drug-Induced Blood Dyscrasias
Practice Questions
Drug-Induced QT Prolongation
Practice Questions
Pharmacovigilance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app