
Drug-Induced QT Prolongation — MCQs

Identify the ECG given below?
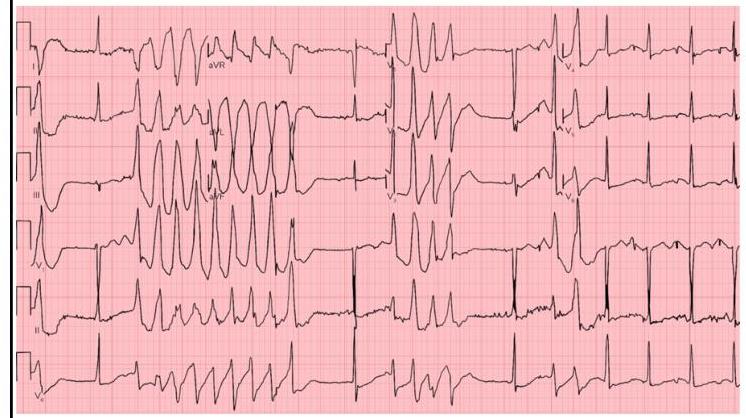
Features of Torsade de pointes include which of the following?
Match the following drugs in Column A with their contraindications in Column B. | Column A | Column B | | :-- | :-- | | 1. Morphine | 1. QT prolongation | | 2. Amiodarone | 2. Thromboembolism | | 3. Vigabatrin | 3. Pregnancy | | 4. Estrogen preparations | 4. Head injury |
QT shortening is associated with which electrolyte imbalance?
Which of the following anti-epileptic drugs has the highest teratogenic potential?
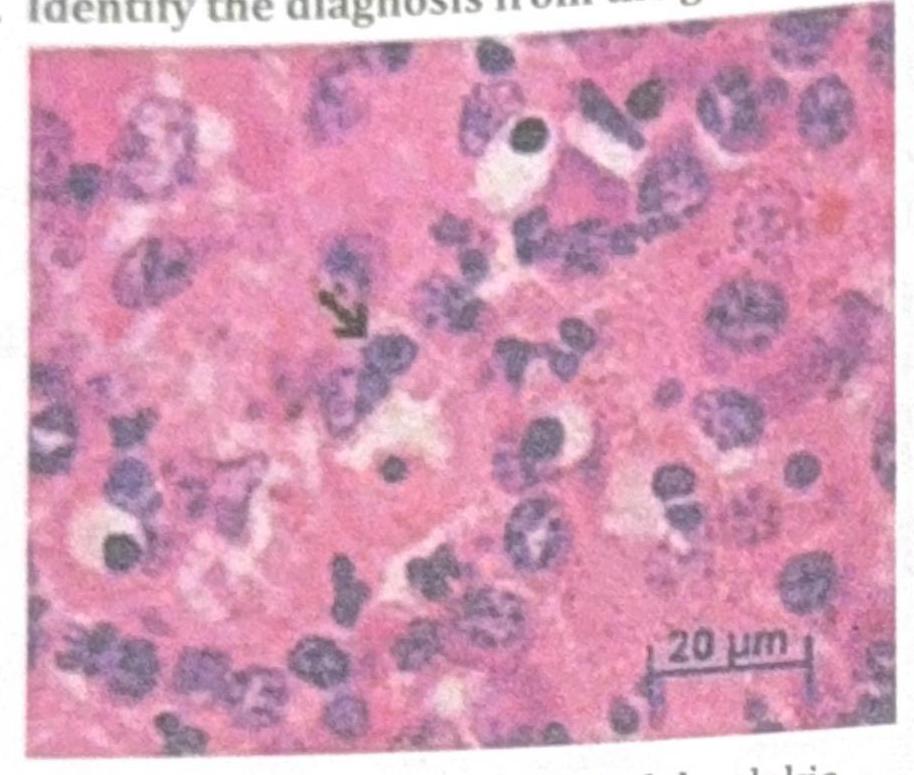
Identify the diagnosis from the given image
Alkaline diuresis in drug poisoning is not done in?
Which one of the following antihypertensive drugs is NOT safe during pregnancy?
Which electrolyte imbalance causes prolonged QT interval?
Which drug should not be given with ketoconazole?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app