
Central Nervous System Pharmacology — MCQs

On this page
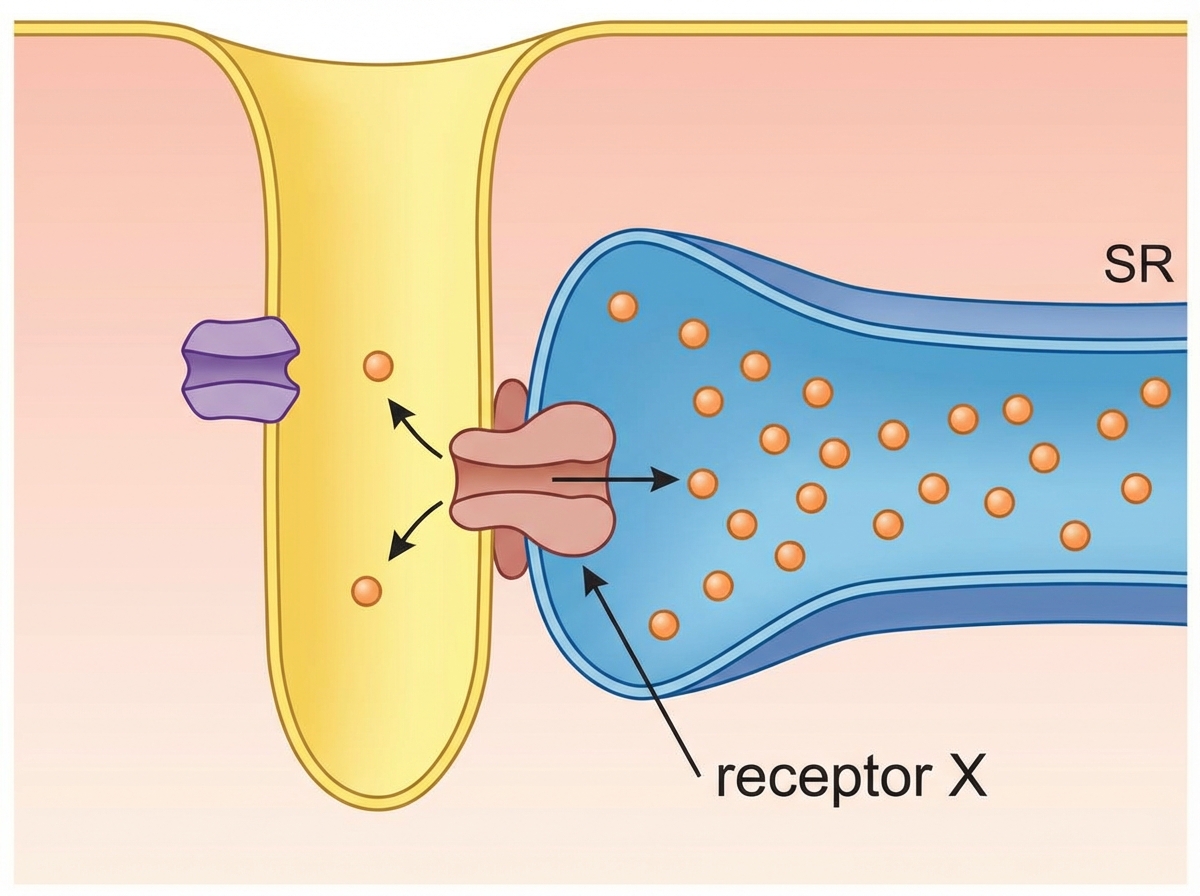
Which drug acts on the receptor X shown below in skeletal muscle?
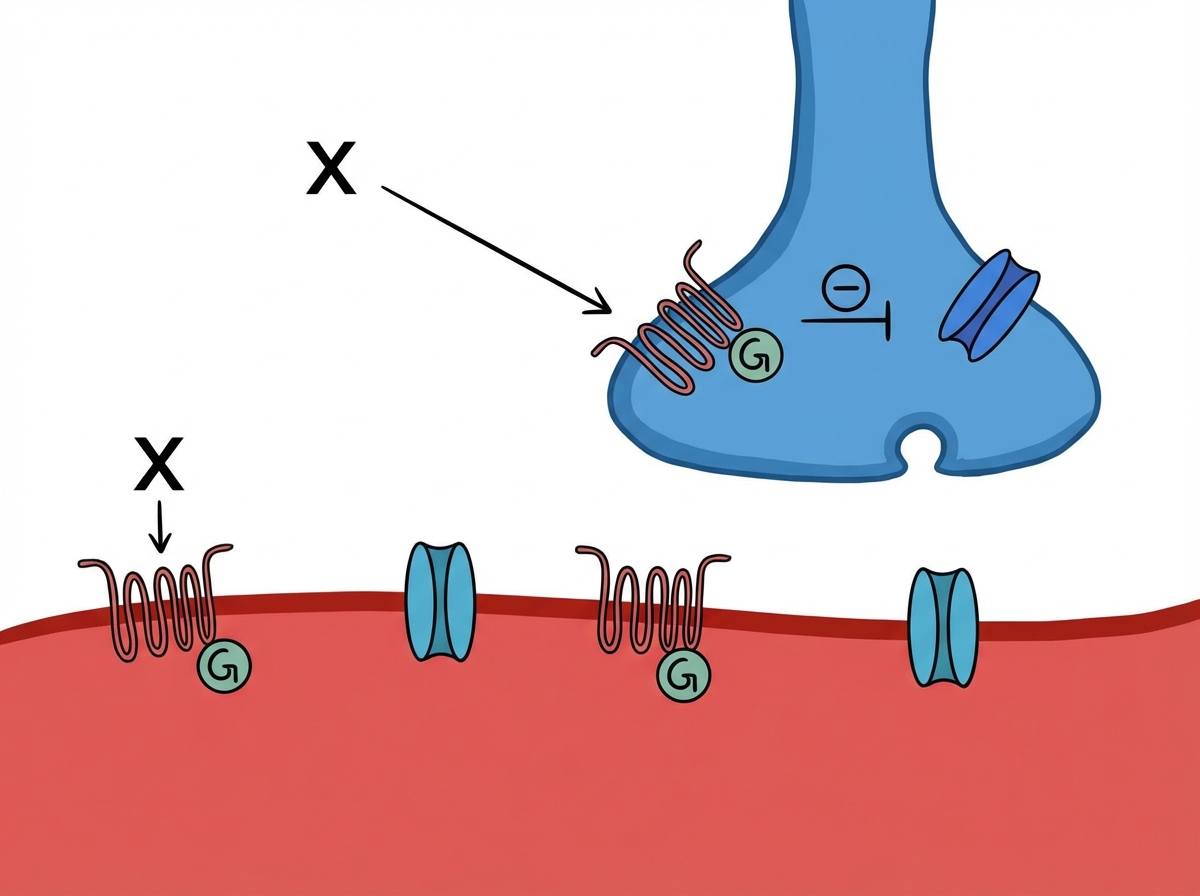
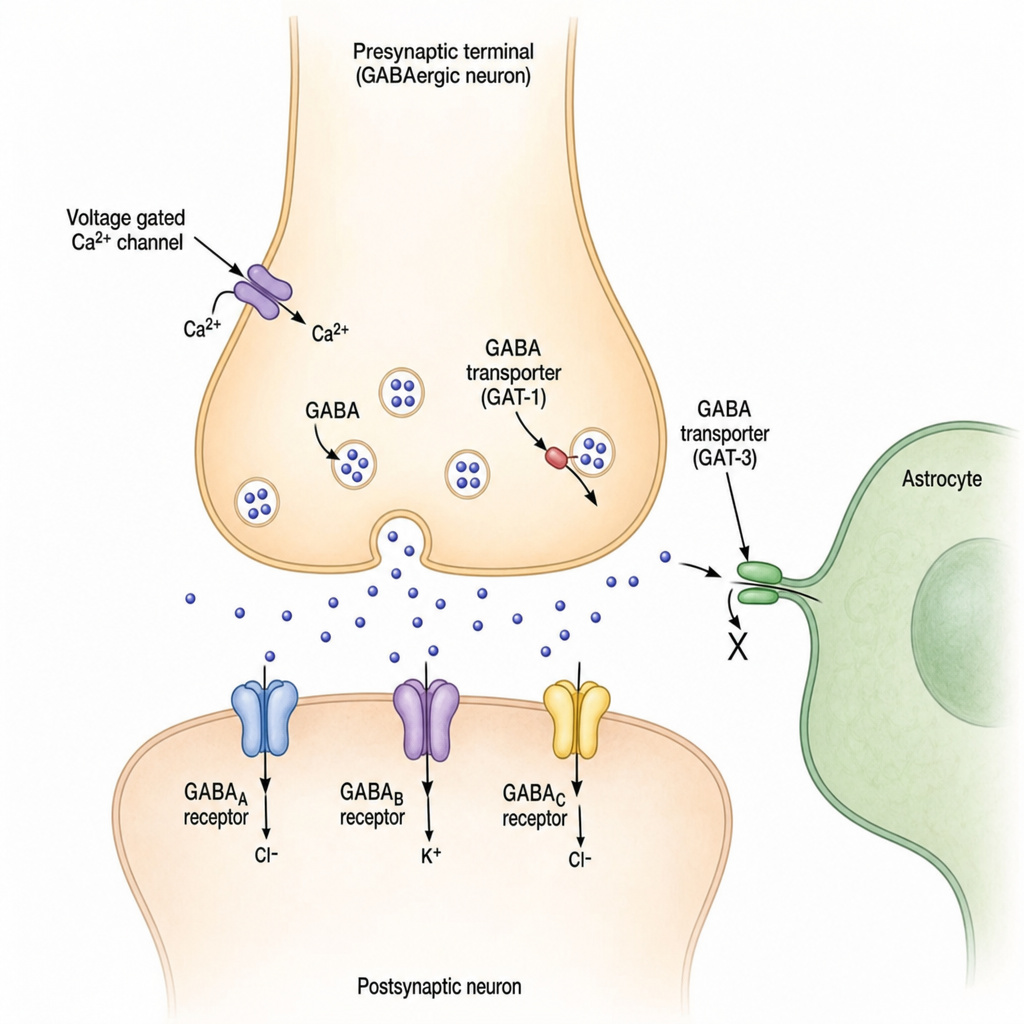
A patient of hemiplegic stroke is having extreme stiffness of arm and truncal musculature. Which drug marked X will act on GABA-B receptors to reduce symptoms? (Recent NEET Pattern 2016-17)
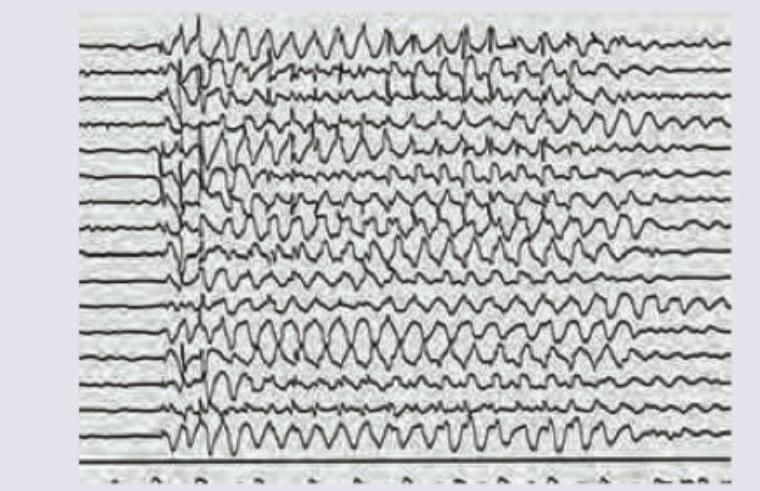
A 6-year-old child has poor school performance. On scolding by teacher abnormal behavior is noted. EEG is performed. Which of the following drugs will cause worsening of the patient?
Which anti-epileptic drug marked X will act at the site shown?
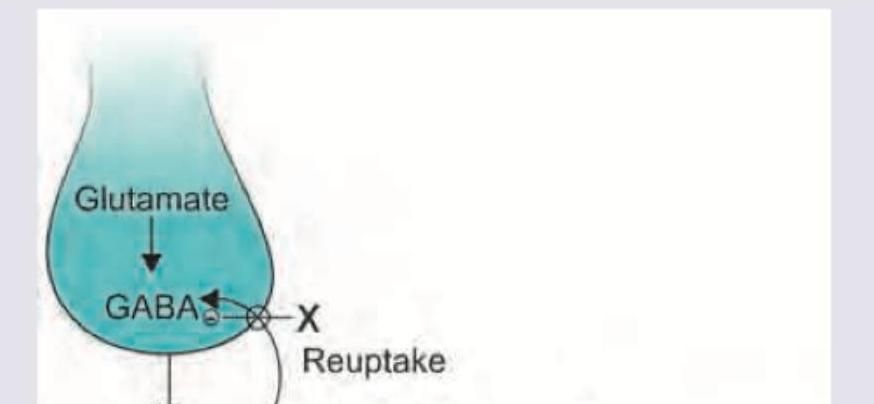
Which anti-epileptic drug marked X will act at the site shown?
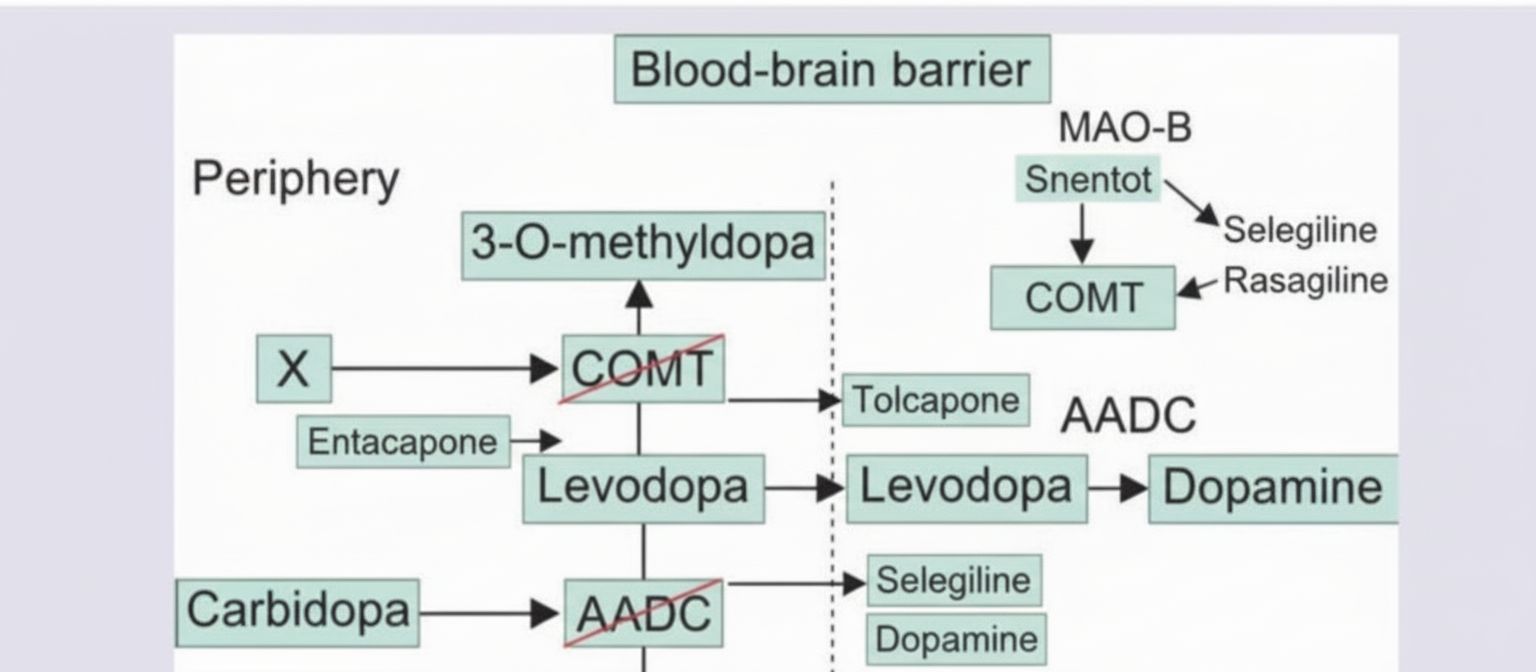
A 70-year-old man is diagnosed with Parkinsonism. Which is the drug at site marked as X?
Which one of the following drugs is a long acting local anaesthetic agent ?
The anticonvulsant of choice in the treatment of generalized tonic-clonic seizures is
Which of the following local anaesthetics causes irreversible cardiac arrest if it is given intravenously ?
The first drug approved for Rett syndrome is?
Practice by Chapter
General Anesthetics
Practice Questions
Local Anesthetics
Practice Questions
Sedative-Hypnotics
Practice Questions
Antiepileptic Drugs
Practice Questions
Antiparkinsonian Drugs
Practice Questions
Opioid Analgesics
Practice Questions
Drugs of Abuse and Addiction
Practice Questions
Psychostimulants
Practice Questions
Hallucinogens
Practice Questions
CNS Stimulants and Cognitive Enhancers
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app