
Central Nervous System Pharmacology — MCQs

On this page
Use of ergotamine is contraindicated in which of the following conditions?
All of the following are true about Triptans except:
Baclofen is used in which of the following conditions?
All of the following statements about phenytoin are true except:
Lorazepam is preferred over Diazepam in the treatment of status epilepticus because:
Which of the following effects is specifically observed with intravenous diazepam and not with other routes of administration?
Which of the following drugs is not metabolized by the liver?
Which of the following does NOT affect the duration of action of local anesthesia?
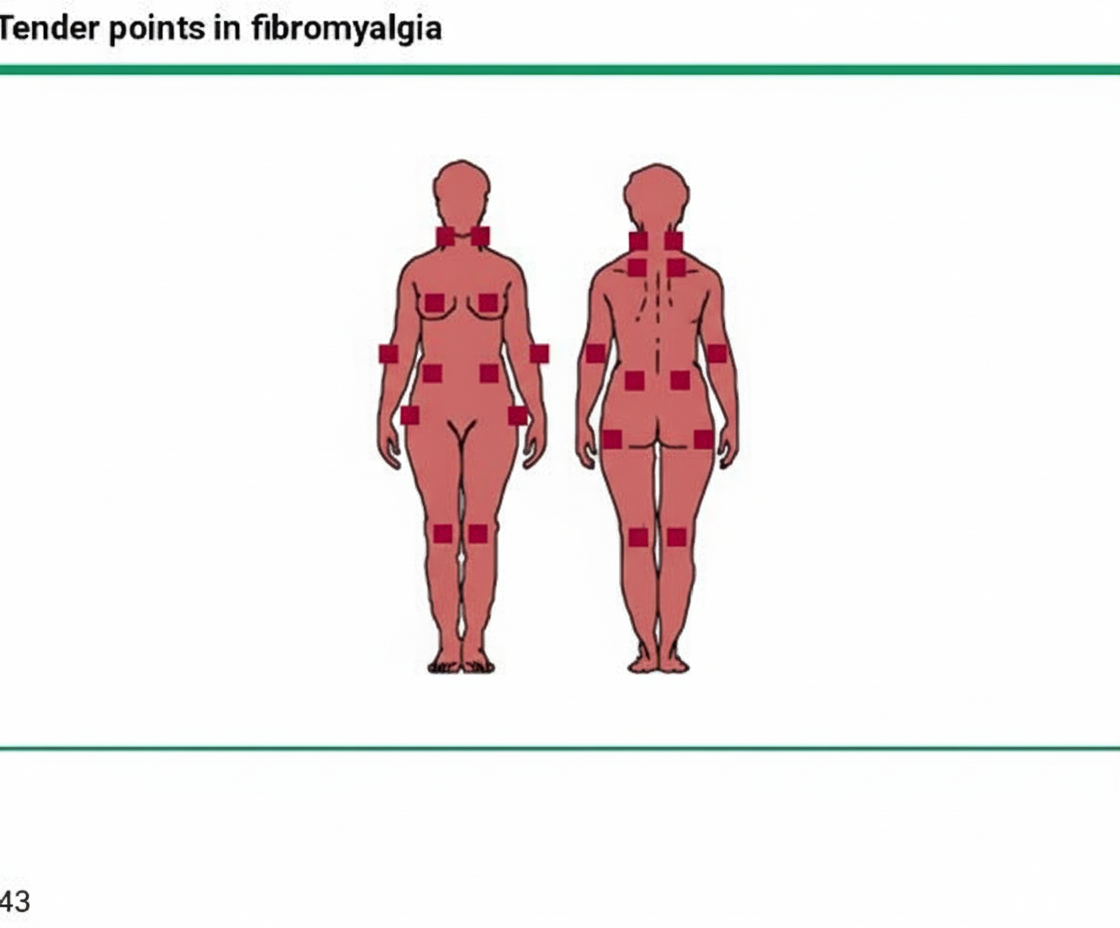
Which serotonin-norepinephrine reuptake inhibitor is predominantly used in the condition shown above?
All of the following drugs are used for managing status epilepticus except?
Practice by Chapter
General Anesthetics
Practice Questions
Local Anesthetics
Practice Questions
Sedative-Hypnotics
Practice Questions
Antiepileptic Drugs
Practice Questions
Antiparkinsonian Drugs
Practice Questions
Opioid Analgesics
Practice Questions
Drugs of Abuse and Addiction
Practice Questions
Psychostimulants
Practice Questions
Hallucinogens
Practice Questions
CNS Stimulants and Cognitive Enhancers
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app