
Cardiovascular Drugs — MCQs

On this page
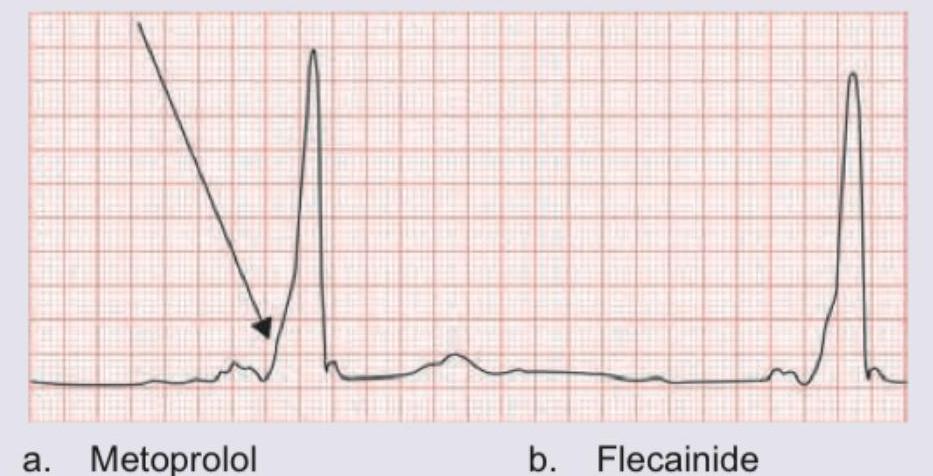
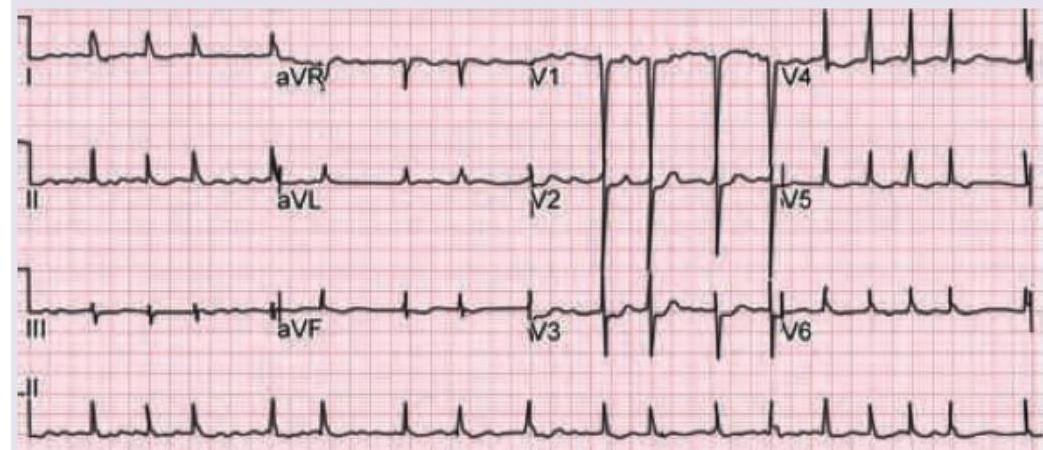
A young air force pilot complains of palpitations and recurrent pre-syncope like condition during training exercises. He passed out in the cockpit in last training exercise after which he is grounded and sent for medical examination. ECG was done. Which of the following drugs is absolutely contraindicated in this condition?
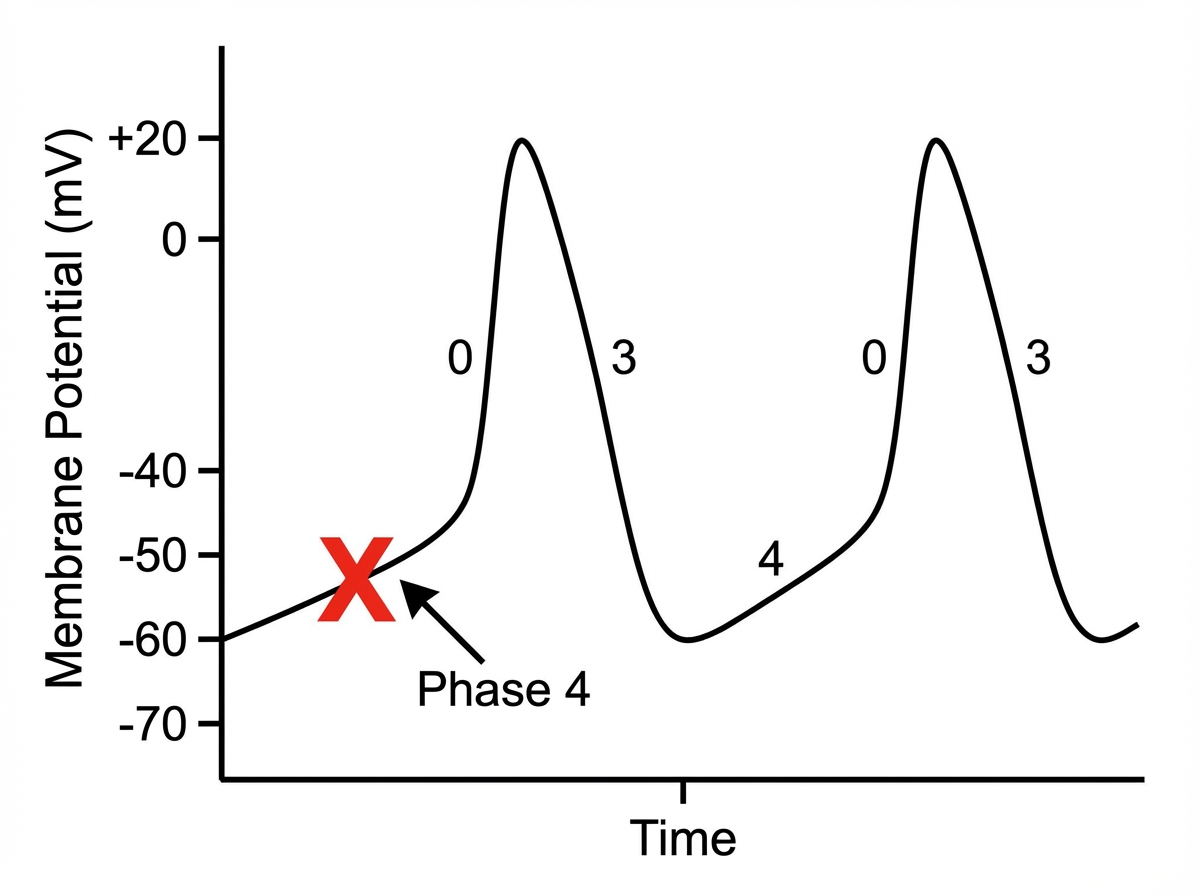
Which of the following drugs will act on the phase of cardiac action potential marked as $X$ ?
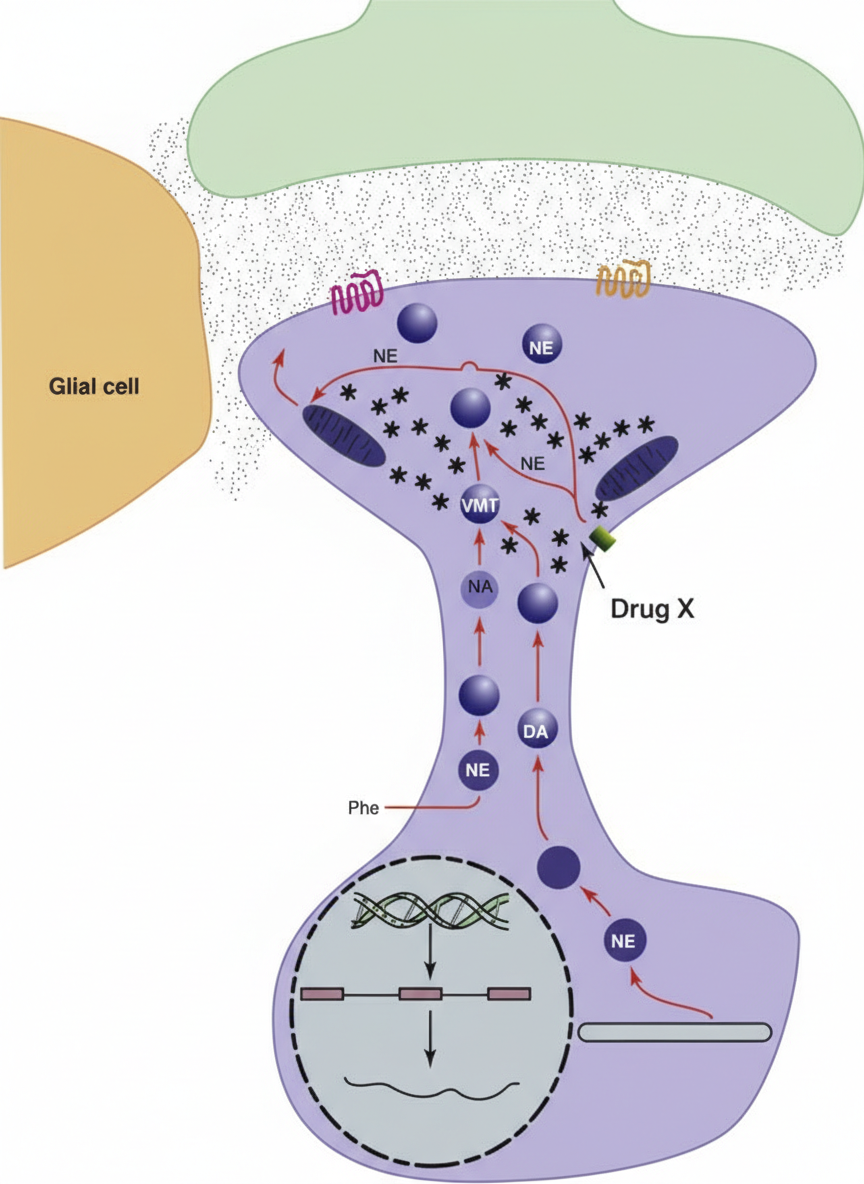
The synaptic cleft shown is from the sympathetic outflow system. The following anti-hypertensive drug $X$ acts via the mechanism shown below:
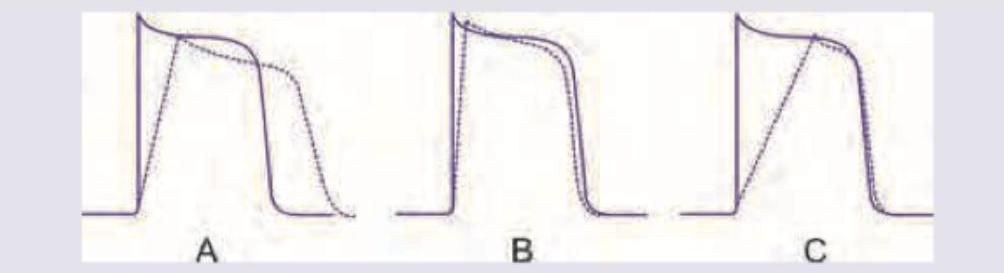
Which of the anti-arrhythmic drug actions shown below will have high predisposition to development of Torsades de pointes?
A 30-year-old male chronic smoker presents with this condition. Which of the following drugs is the preferred drug for improving circulation?

A 50-year-old woman with rheumatic heart disease is on medication for heart disease. She feels unwell for most part of the day. Which of the following medicine is responsible for the ECG changes shown below? (Recent NEET Pattern 2016-17)
Which one of the following responses to intravenous adenosine is correctly matched?
Which of the following anti-hypertensive drugs is/are best avoided during pregnancy ?
Match the following antiarrhythmic drugs with their mechanism of action: | Mechanism of action | Drug | | :-- | :-- | | 1. Na+ channel blocker | A. Quinidine | | 2. K+ channel blocker | B. Digoxin | | 3. Na+K+ ATPase inhibitor | C. Esmolol | | 4. Beta-blocker | D. Ibutilide |
Identify the correct match, regarding the drug and its adverse effect.
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app