
Cardiovascular Drugs — MCQs

On this page
Which of the following is not true regarding bempedoic acid?
Mechanism of action of Fenoldopam drug is:
A patient with recurrent episodes of PSVT (Paroxysmal Supraventricular Tachycardia) is being considered for long-term prophylactic therapy to prevent future episodes. Which of the following is the most appropriate preventive treatment?
A patient with paroxysmal supraventricular tachycardia (PSVT) requires treatment for prophylaxis. Which drug is appropriate?
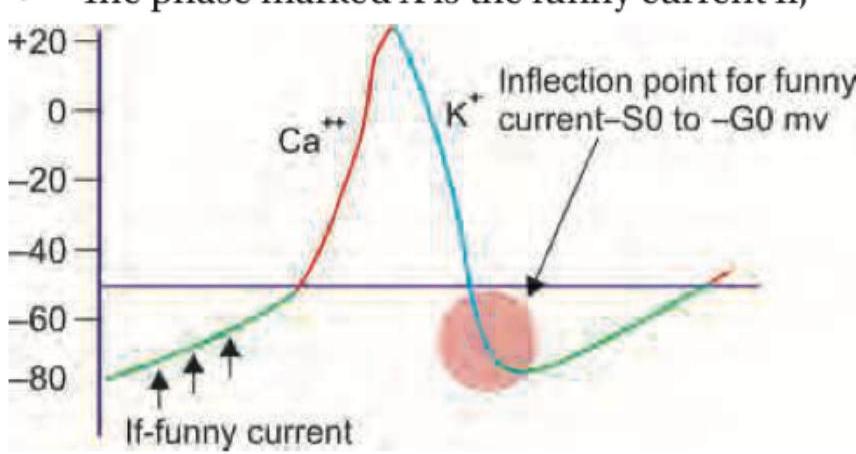
The image above (labeled img-78.jpeg) shows a cardiac action potential. The phase marked X represents the funny current (If). Which drug selectively blocks this funny current and is used in chronic CHF and chronic stable angina?
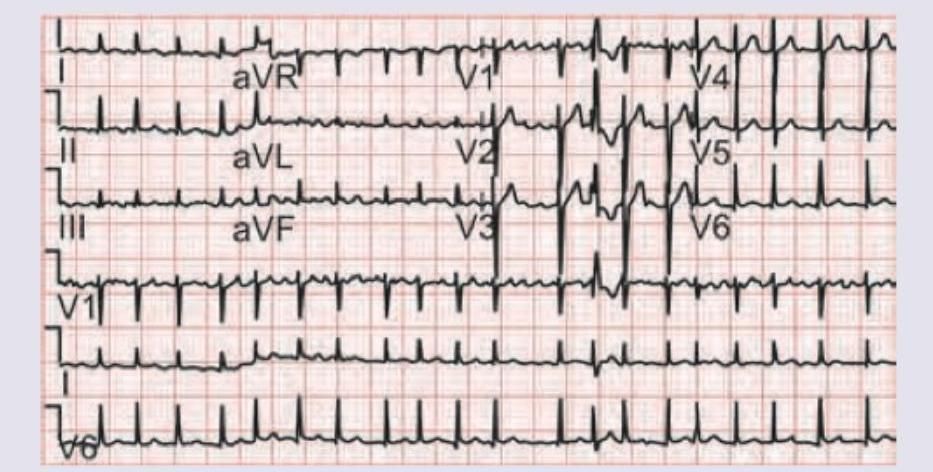
A 65-year-old retired school teacher presents with chest pain of 6 hours duration with dyspnea grade III. On examination RR $=24 / \mathrm{min}$ with use of accessory muscles of respiration, elevated pulsatile JVP, pulse rate of 120 bpm and $\mathrm{BP}=150 / 90$. Troponin I is $0.08 \mathrm{ng} / \mathrm{dL}$ and ECG is shown below. Which of these drugs will not be useful for this patient?

A 50-year-old patient with premature atherosclerosis has deranged lipid profile. On examination there is development of plane xanthomas in palmar creases. All are useful for this patient except:
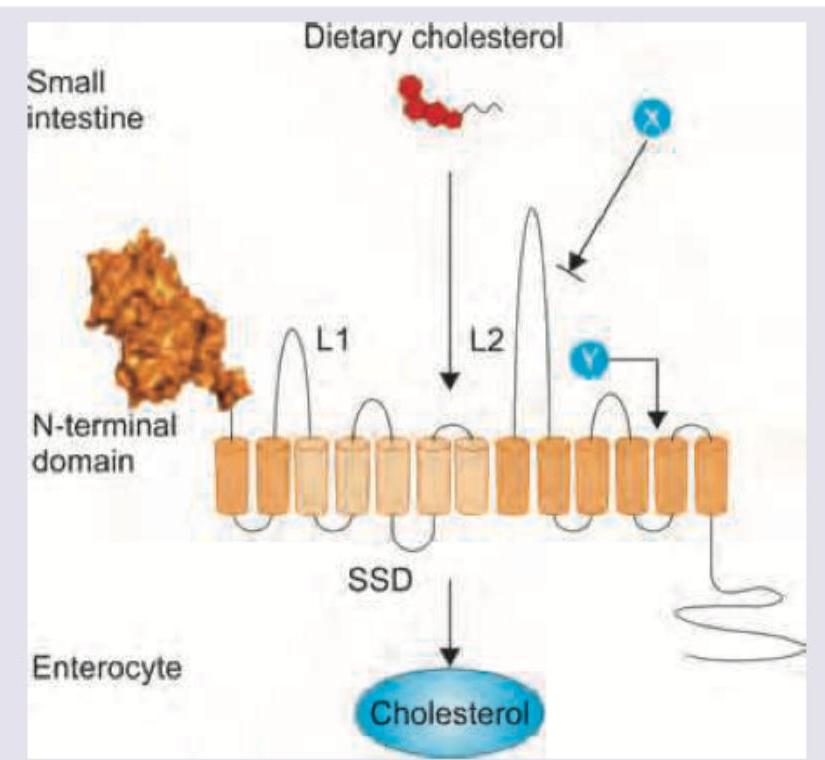
A 50-year-old patient with type IIA hyperlipoproteinemia is started on intestinal cholesterol absorption inhibitor. Which drug and its receptor combination is correct?
A 60-year-old hypertension patient presents with palpitations and pre-syncope. ECG was done. All drugs can be used for management of this condition except:
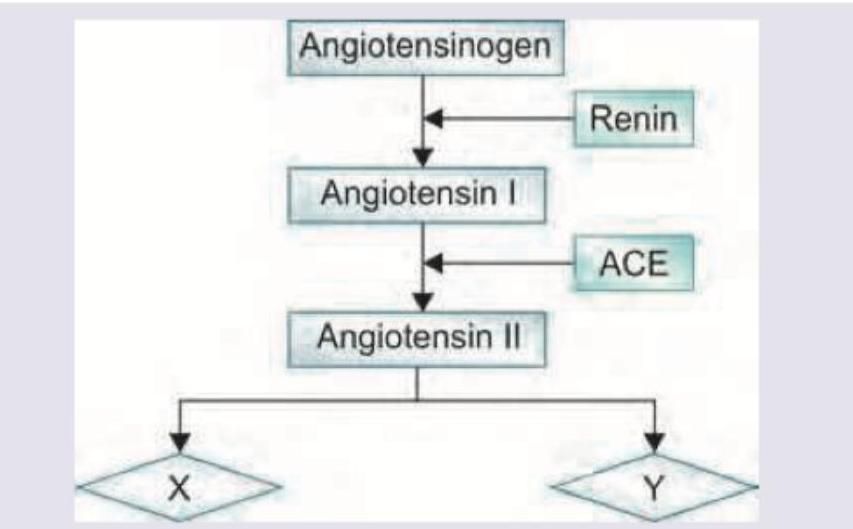
Telmisartan acts on the following receptors for its action. Name X and Y? (Recent NEET Pattern 2016-17)
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app