
Cardiovascular Drugs — MCQs

On this page
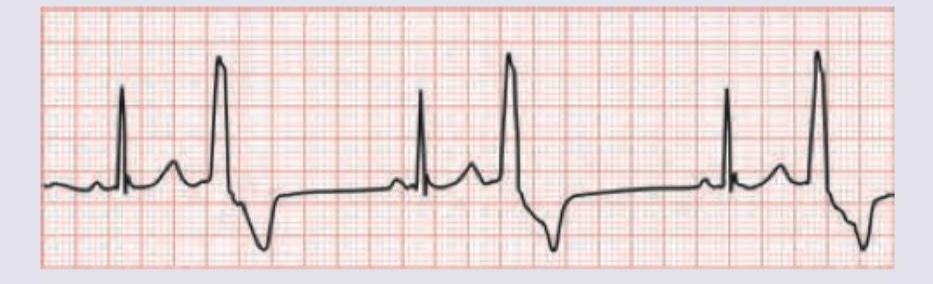
A 65-year-old retired school teacher presents with chest pain of 6 hours duration with dyspnea grade III. On examination RR $=24 / \mathrm{min}$ with use of accessory muscles of respiration, elevated pulsatile JVP, pulse rate of 120 bpm and $\mathrm{BP}=150 / 90$. Troponin I is $0.08 \mathrm{ng} / \mathrm{dL}$ and ECG is shown below. Which of these drugs will not be useful for this patient?

Prescription of which of the following drugs can lead to periorbital edema of non-pitting variety?
A 50-year-old patient with premature atherosclerosis has deranged lipid profile. On examination there is development of plane xanthomas in palmar creases. All are useful for this patient except:
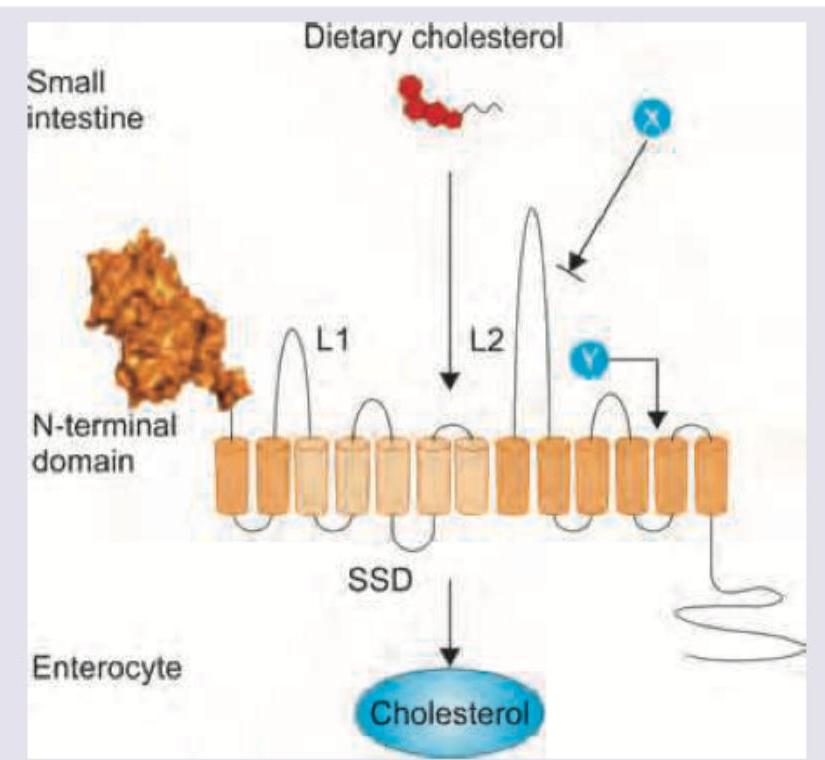
A 50-year-old patient with type IIA hyperlipoproteinemia is started on intestinal cholesterol absorption inhibitor. Which drug and its receptor combination is correct?
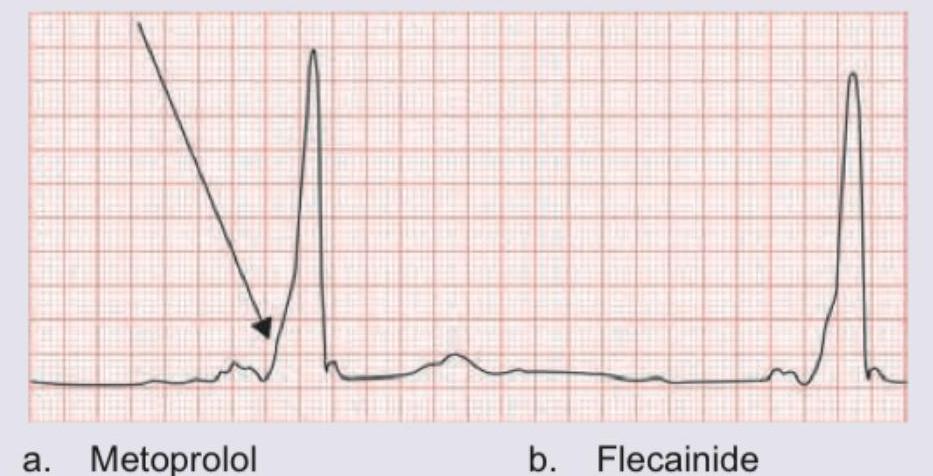
A 1-year-old child with moderate VSD is scheduled for surgery next month. For control of symptoms of CHF, a drug $X$ was given. The uneducated parents gave double the dose of drug resulting in the child developing listlessness and poor feeding. Based on the ECG shown, what is the drug prescribed and its side effect?
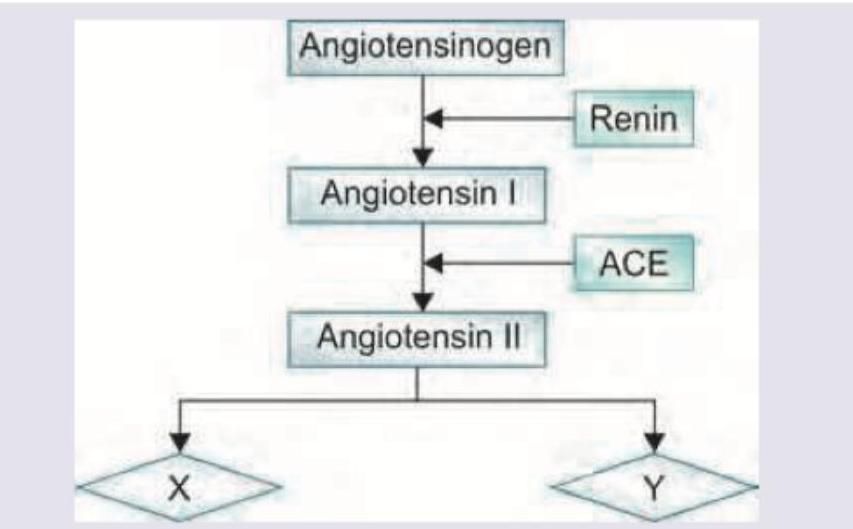
Telmisartan acts on the following receptors for its action. Name X and Y? (Recent NEET Pattern 2016-17)
A young air force pilot complains of palpitations and recurrent pre-syncope like condition during training exercises. He passed out in the cockpit in last training exercise after which he is grounded and sent for medical examination. ECG was done. Which of the following drugs is absolutely contraindicated in this condition?
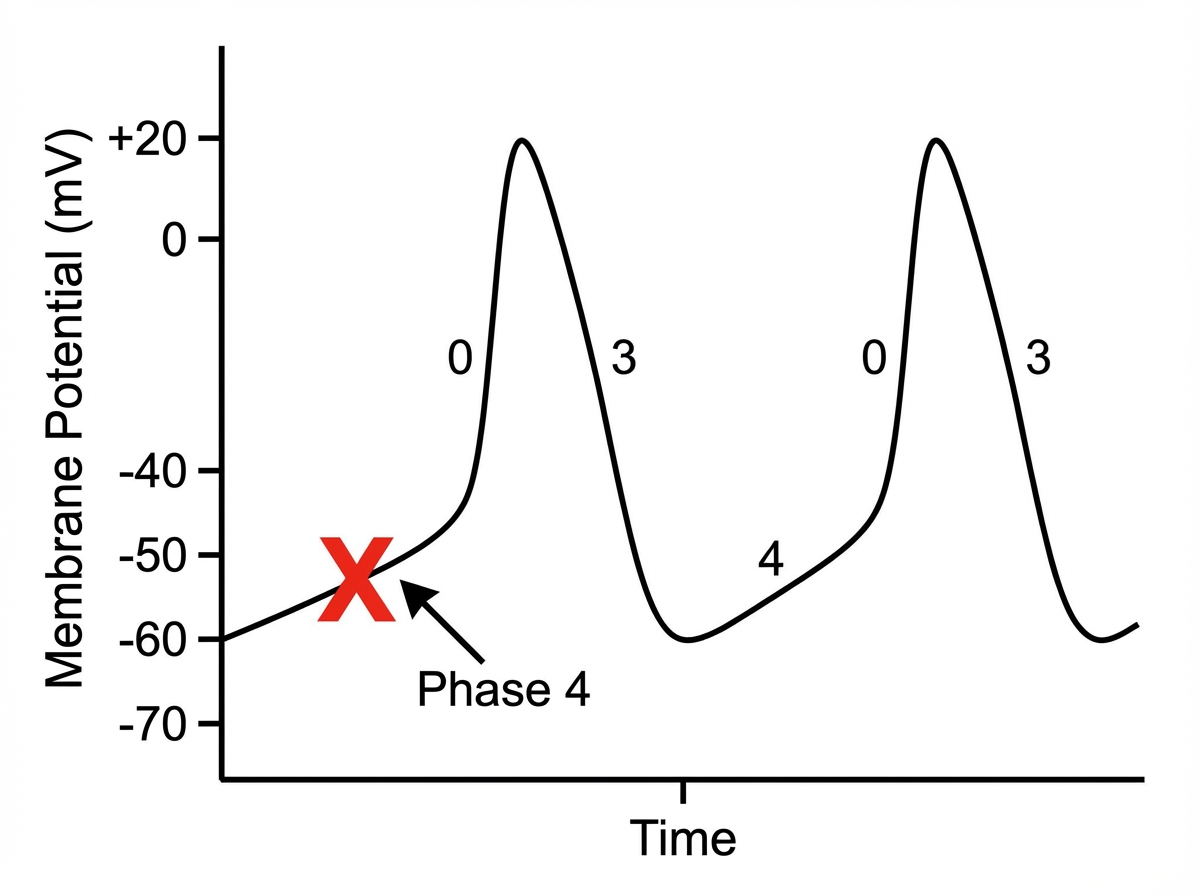
Which of the following drugs will act on the phase of cardiac action potential marked as $X$ ?
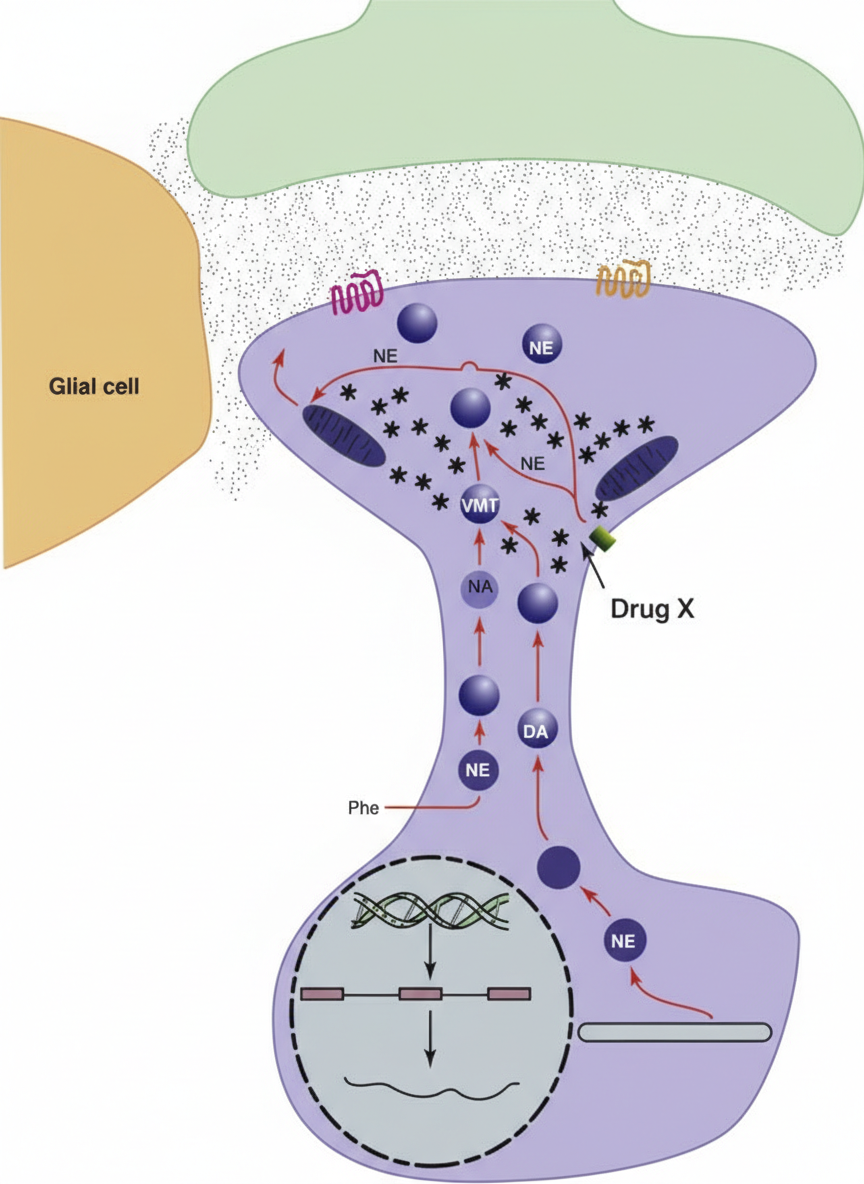
The synaptic cleft shown is from the sympathetic outflow system. The following anti-hypertensive drug $X$ acts via the mechanism shown below:
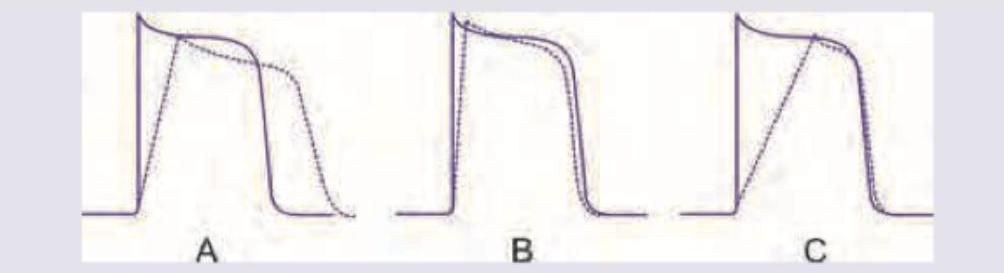
Which of the anti-arrhythmic drug actions shown below will have high predisposition to development of Torsades de pointes?
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app