
Cardiovascular Drugs — MCQs

On this page
What are the most potent drugs for reducing plasma cholesterol levels?
Which of the following drugs is commonly associated with causing a cough?
A patient on antihypertensive medication develops a dry cough. Which of the following drugs might be responsible for this condition?
A patient with hypertension, tachycardia and early renal involvement is prescribed an ARB (telmisartan). What is the most likely mechanism by which the drug helps improve heart rate and blood pressure?
A patient with a history of hypertension is given the drug 'X'. Identify 'X'?
Which of these drugs stimulates PPAR-alpha (Peroxisome proliferator-activated receptor alpha)?
A patient with atrial fibrillation is started on a medication that prolongs the QT interval by blocking potassium channels. Which of the following is the most likely adverse effect of this antiarrhythmic drug?
Which of the following is not true regarding bempedoic acid?
Mechanism of action of Fenoldopam drug is:
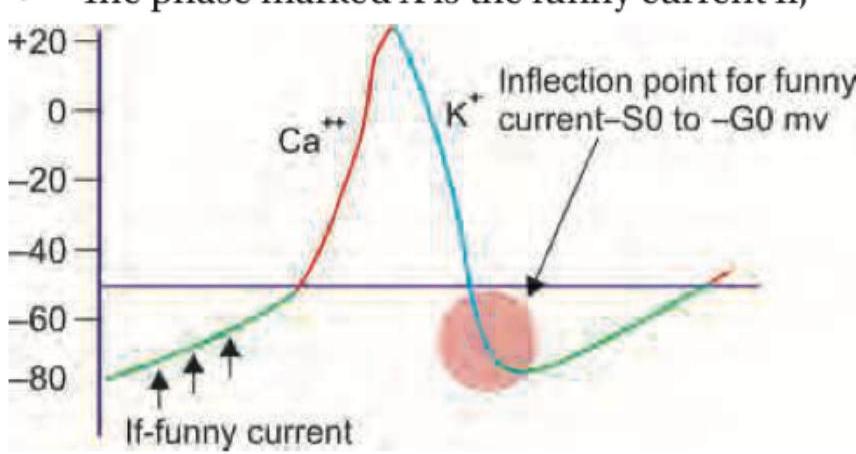
The image above (labeled img-78.jpeg) shows a cardiac action potential. The phase marked X represents the funny current (If). Which drug selectively blocks this funny current and is used in chronic CHF and chronic stable angina?
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app