
Cardiovascular Drugs — MCQs

On this page
Dobutamine is preferred over Dopamine in cardiogenic shock because of its effects related to what?
Angiotensin converting enzyme inhibitors are useful in congestive heart failure as:
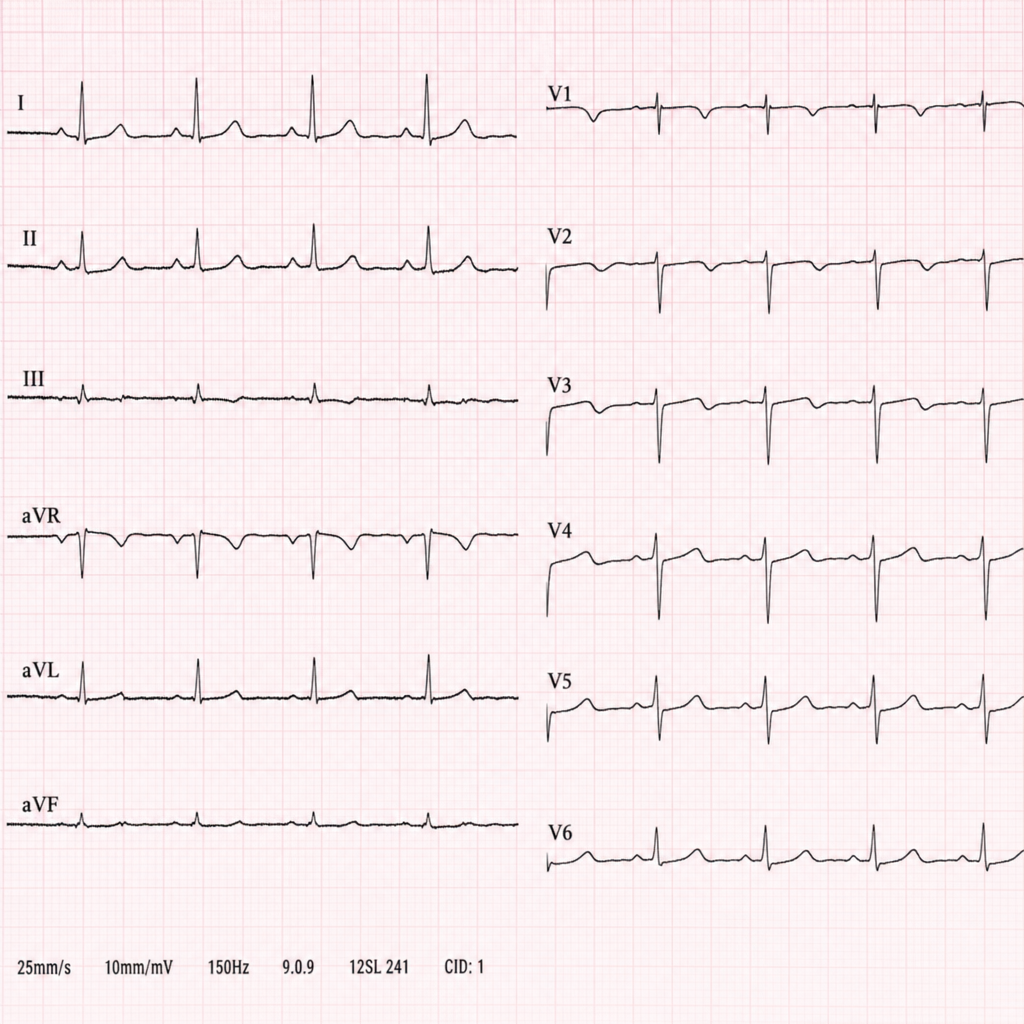
A 50-year-old male presented with the following ECG pattern. Which drug should not be given for his condition?
Alprostadil is not used for the treatment of which of the following conditions?
Which antiarrhythmic drug can be used for arrhythmias refractory to lignocaine treatment?
Niacin must be used cautiously in diabetic patients because?
Which drug class inhibits the rate-limiting step in cholesterol synthesis?
Nitrate causes all of the following EXCEPT:
Riociguat is used in the treatment of:
A diabetic patient with bilateral renal artery stenosis requires a drug for the treatment of high blood pressure. Which of the following drugs will be most appropriate for this patient?
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app