
Cardiovascular Drugs — MCQs

On this page
Ivabradine is used for the management of which condition?
Calcium dobesilate is used in the treatment of varicose veins because of which of the following mechanisms, except:
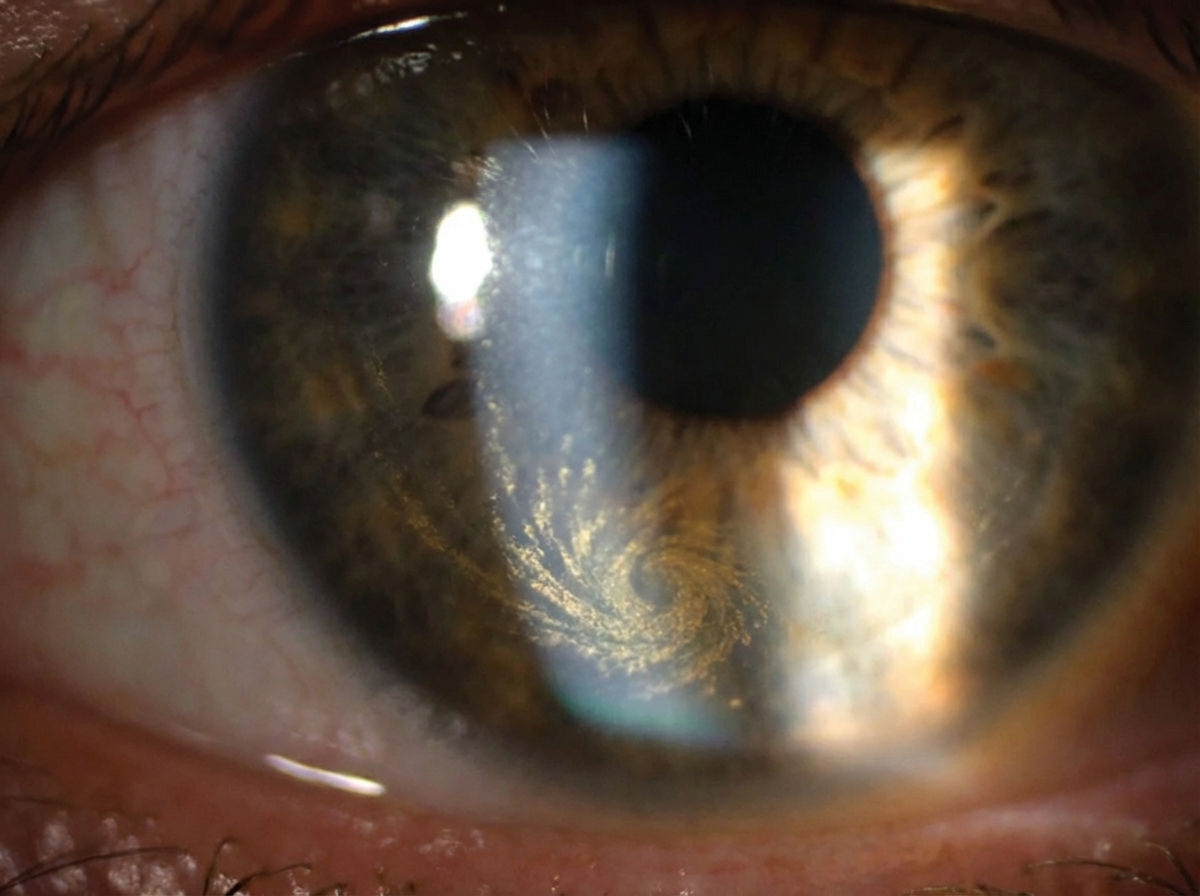
A 55-year-old cardiac patient on long-term treatment presents for a follow-up visit. The physician observes a specific finding on ophthalmological examination. Which drug prescribed by the physician is most likely responsible for this finding?
Which drug is contraindicated in bilateral renal artery stenosis?
Sudden withdrawal of which of the following drugs could result in serious adverse cardiovascular changes in a patient taking the drug over a long time?
What is the biochemical mechanism of action of digitalis?
Which of the following is NOT true about fibrates?
Enalapril increases the levels of which of the following?
All of the following drugs can be used in hypertensive crisis except?
Which statin is not metabolized by CYP3A4?
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app