
Cardiovascular Drugs — MCQs

On this page
Which of the following changes in ECG is most commonly associated with Digitalis use?
Which drug decreases lipoprotein(a) in the blood?
Skin blood flow is decreased by ?
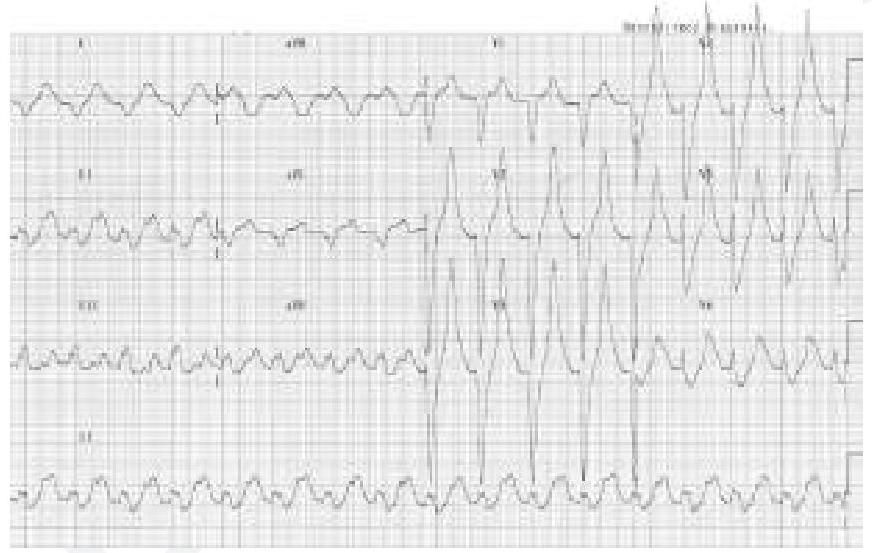
A patient who is a known case of hypertension on multiple anti-hypertensive medications came to OPD. His ECG finding is given below. Which of the following drugs is responsible for the ECG finding? (Image of ECG finding)
What is the primary mechanism of action of beta-blockers in the management of hypertension?
Which of the following drugs can be given in patients of primary pulmonary hypertension?
Endothelin primarily acts through which type of receptors?
What is the drug of choice for treating tachycardia induced by digitalis?
What is the primary function of PGI2?
What type of drug is Sacubitril?
Practice by Chapter
Antihypertensive Agents
Practice Questions
Drugs for Heart Failure
Practice Questions
Antiarrhythmic Drugs
Practice Questions
Antianginal Agents
Practice Questions
Lipid-Lowering Drugs
Practice Questions
Anticoagulants and Antiplatelet Drugs
Practice Questions
Thrombolytic Agents
Practice Questions
Drugs Used in Pulmonary Hypertension
Practice Questions
Drugs Used in Shock
Practice Questions
Cardiovascular Effects of Non-Cardiovascular Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app