
Antimicrobial Agents — MCQs

On this page
Which of the following is the treatment for complicated gonorrhoea due to penicillin-resistant Neisseria gonorrhoeae?
Which of the following is the classical drug for clinical cure in malaria?
A male patient with a history of MSM presents with urethral discharge. There is penicillin resistance on testing. Which drug should be given?
Patient came with fever headache and nuchal rigidity. LP shows gram-negative diplococci in gram stain. Which of the following will be used for chemoprophylaxis in close contacts of a patient with meningococcal meningitis?
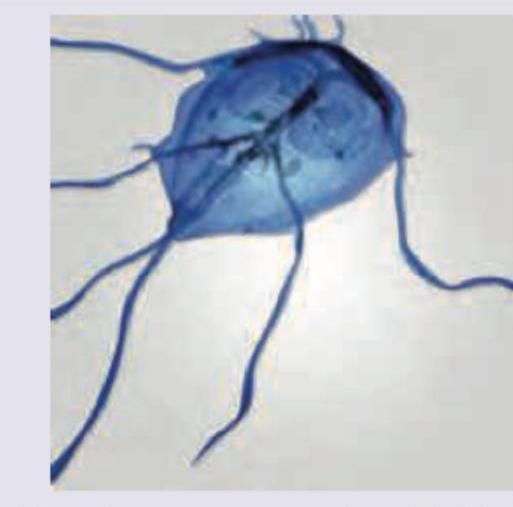
All are used in treatment for the GIT parasite shown below except:
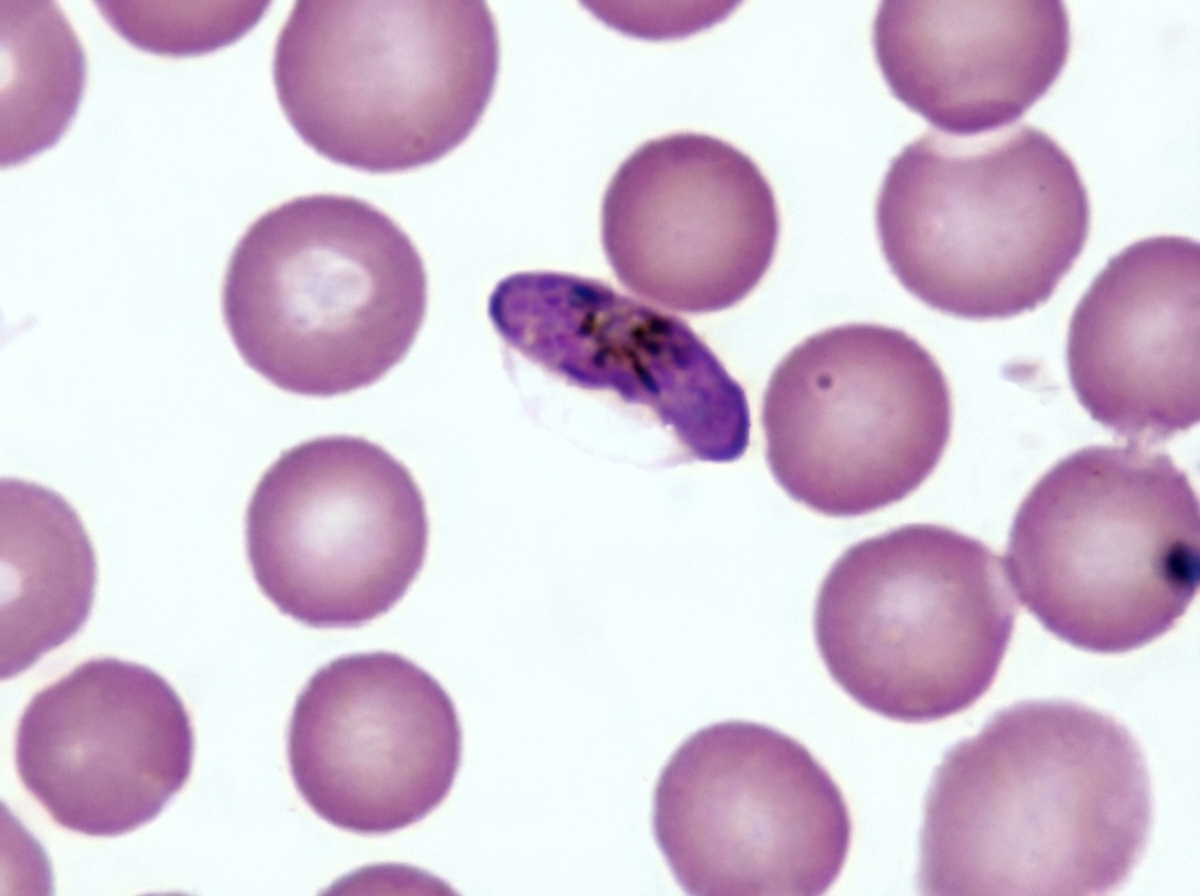
All of the following drugs will act on the mature stage V gametocytes of Plasmodium falciparum except:
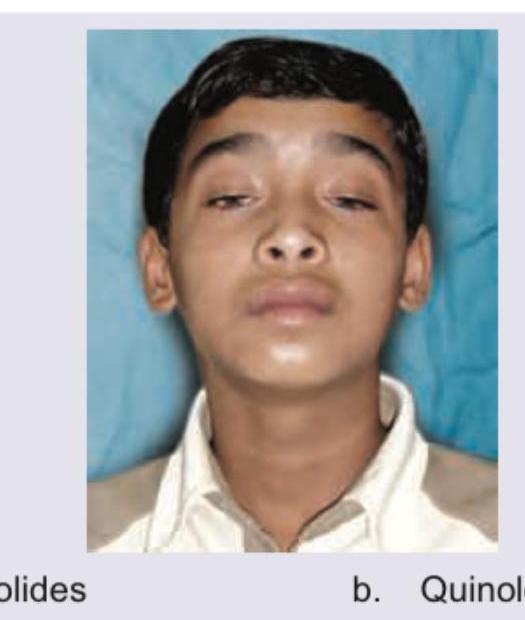
Based on the above diagnosed patient of Myasthenia Gravis, which of the following antibiotics is LEAST likely to exacerbate the condition?
A 30-year-old patient from a rural area presents with right upper quadrant pain, fever, and marked eosinophilia. He reports a history of consuming raw watercress from a local stream. Stool examination reveals the organism shown in the image below. What is the drug of choice for this infection?

A 24-year-old patient presents with a 1-week history of vulvar itching and vaginal discharge. She says that she has had intercourse with two individuals in the past 6 months without the use of a condom. On physical examination, the vulva is edematous. Discharge is present on the vaginal walls and at the cervical os. Wet smear of vaginal secretions shows epithelial cells, white blood cells, and flagellate protozoa. You prescribe an antibiotic. What warning do you give about this particular treatment?
Daily suppressive therapy for HSV-1 and HSV-2 is :
Practice by Chapter
Beta-Lactam Antibiotics
Practice Questions
Aminoglycosides
Practice Questions
Macrolides and Ketolides
Practice Questions
Tetracyclines
Practice Questions
Quinolones
Practice Questions
Sulfonamides and Trimethoprim
Practice Questions
Antimycobacterial Drugs
Practice Questions
Antifungal Agents
Practice Questions
Antiviral Drugs
Practice Questions
Antiparasitic Agents
Practice Questions
Principles of Antimicrobial Selection
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app