
Antimicrobial Agents — MCQs

On this page
Ichthyosis is a side effect of -
Drug that is contraindicated in renal failure is:
Pseudotumor Cerebri in Infants is seen with?
Which of the following is true about Mafenide?
Treatment of choice for chloroquine resistant malaria is :
What is false about mafenide acetate?
Which of the following produces neuropsychiatric symptoms?
Which of the following is/are 1st line antitubercular drugs for children?
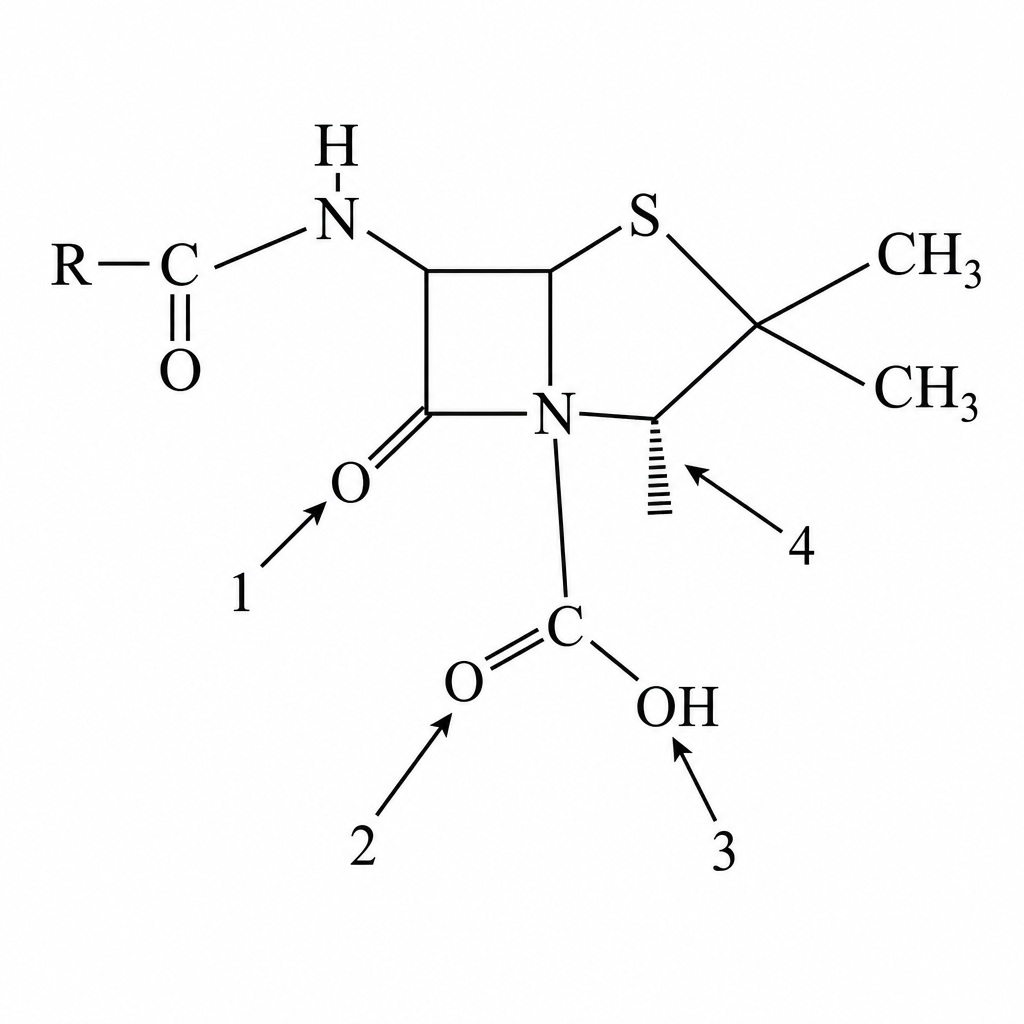
A 28-year-old female with folliculitis is not responsive to a 10-day treatment course with penicillin. An enzyme produced by the etiologic agent is most likely responsible for this treatment failure. At which site on the molecule shown does this enzyme act to destroy penicillin?
Red man syndrome occurs with :
Practice by Chapter
Beta-Lactam Antibiotics
Practice Questions
Aminoglycosides
Practice Questions
Macrolides and Ketolides
Practice Questions
Tetracyclines
Practice Questions
Quinolones
Practice Questions
Sulfonamides and Trimethoprim
Practice Questions
Antimycobacterial Drugs
Practice Questions
Antifungal Agents
Practice Questions
Antiviral Drugs
Practice Questions
Antiparasitic Agents
Practice Questions
Principles of Antimicrobial Selection
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app