
Antimicrobial Agents — MCQs

On this page
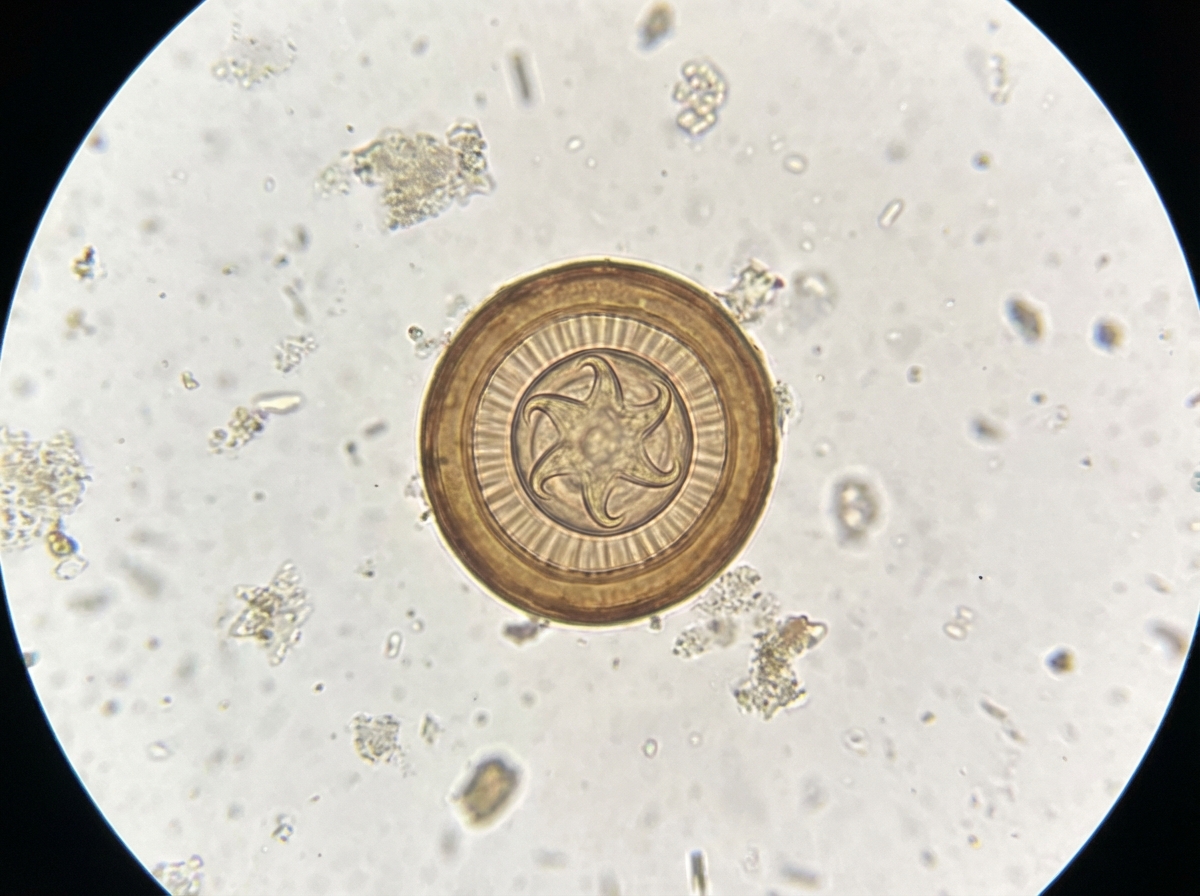
A 10-year-old child presents with diarrhea and abdominal pain for 4 days. Stool microscopy reveals findings suggestive of a parasitic infection. Which of the following medications is indicated for treatment?
Which of the following inhibitors of protein synthesis is primarily bactericidal?
Metronidazole is used for all of the following conditions except:
All of the following are true of pyrazinamide EXCEPT?
Which drugs are safe in pregnancy for a patient with HIV infection?
Which of the following antifungal drugs is NOT used in the treatment of intestinal candidiasis?
Ethambutol toxicity is most commonly associated with visual disturbances. Which color vision deficiency is characteristic of ethambutol toxicity?
Which of the following antiviral drugs is used against HCV infection?
Which of the following is used for single dose radical cure of Plasmodium vivax malaria?
Tetracycline is contraindicated in:
Practice by Chapter
Beta-Lactam Antibiotics
Practice Questions
Aminoglycosides
Practice Questions
Macrolides and Ketolides
Practice Questions
Tetracyclines
Practice Questions
Quinolones
Practice Questions
Sulfonamides and Trimethoprim
Practice Questions
Antimycobacterial Drugs
Practice Questions
Antifungal Agents
Practice Questions
Antiviral Drugs
Practice Questions
Antiparasitic Agents
Practice Questions
Principles of Antimicrobial Selection
Practice Questions
Antimicrobial Resistance
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app