
Macrolides and Ketolides — MCQs

Which of the following is NOT a mechanism of antibiotic resistance?
What is the mechanism of action of aminoglycoside antibiotics?
What is the mechanism of resistance in MRSA?
Which of the following antimicrobials should not be given to a chronic asthmatic patient managed on theophylline therapy?
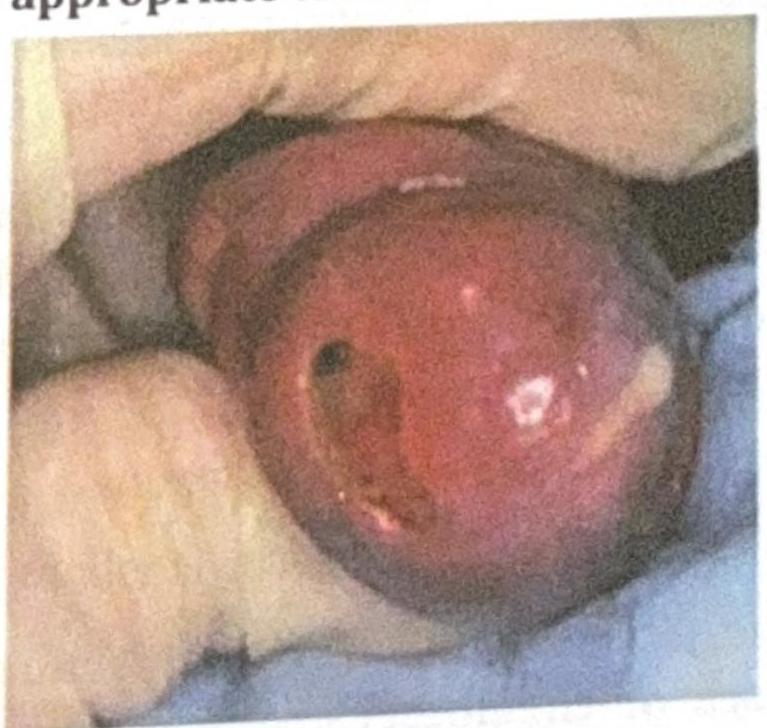
An adult man presents with the clinical condition shown in the image, and a Gram stain reveals Gram-negative diplococci. What is the most appropriate treatment?
Which one of the following antibiotics inhibits transpeptidation in bacterial cell wall synthesis?
Which of the following combinations can result in severe toxicity due to inhibition of cytochrome P450 enzymes?
Why does Mycoplasma genitalium show a higher rate of antimicrobial resistance compared to other STI pathogens?
A 14-year-old boy presents with headache, fever, and cough for 2 days. Sputum is scant and non-purulent and gram stain reveals many white cells but no organisms. The treatment should be initiated with :
What is the drug that can be used for rheumatic fever prophylaxis in a patient with a history of allergy to Penicillin?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app