
Anticancer Drugs — MCQs

On this page
Treatment with Herceptin in breast cancer is indicated for
Herceptin (Trastuzumab) is an immunotherapeutic agent used in the treatment of:
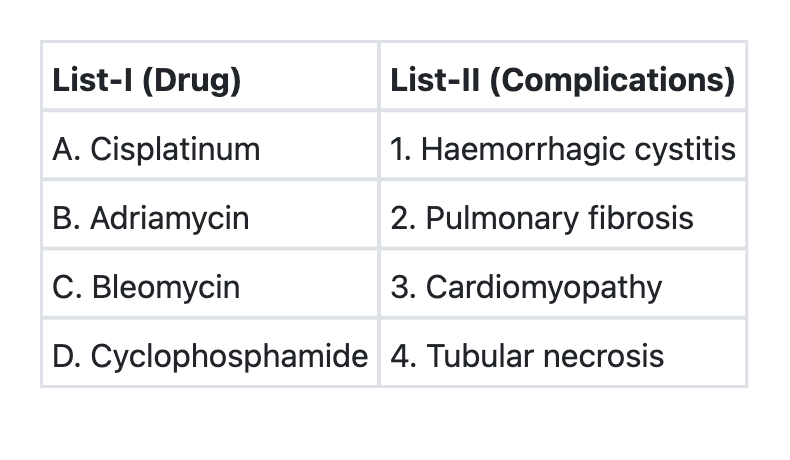
Match List-I with List-II and select the correct answer using the code given below the Lists:
Which of the following are the vaccines for prevention of cervical cancer? 1. Cervarix 2. Gardasil 3. T-dap 4. Influenza Select the correct answer using the code given below:
All of the following are hormonal agents used in treatment of cancer EXCEPT:
Match the following drugs with the targets of their actions: Drugs: A. Trastuzumab B. Infliximab C. Sirolimus D. Imatinib Targets: 1. BCR-ABL tyrosine kinase 2. mTOR 3. TNF alpha 4. HER2/neu
A lady who had undergone mastectomy for breast cancer is being treated with tamoxifen. How long should it be stopped before she can conceive?
Which among the following drugs is the new FDA approved immune checkpoint inhibitor for endometrial carcinoma?
Osimertinib is used in NSCLC with which mutation?
What is the treatment for HER-2 positive trastuzumab resistant breast cancer?
Practice by Chapter
Principles of Cancer Chemotherapy
Practice Questions
Alkylating Agents
Practice Questions
Antimetabolites
Practice Questions
Antitumor Antibiotics
Practice Questions
Plant Alkaloids
Practice Questions
Topoisomerase Inhibitors
Practice Questions
Hormonal Agents
Practice Questions
Targeted Therapy
Practice Questions
Immunotherapy
Practice Questions
Management of Chemotherapy Side Effects
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app