
Anticancer Drugs — MCQs

On this page
Which of the following parameters is not monitored in a patient on methotrexate therapy?
Which of the following causes peripheral neuritis?
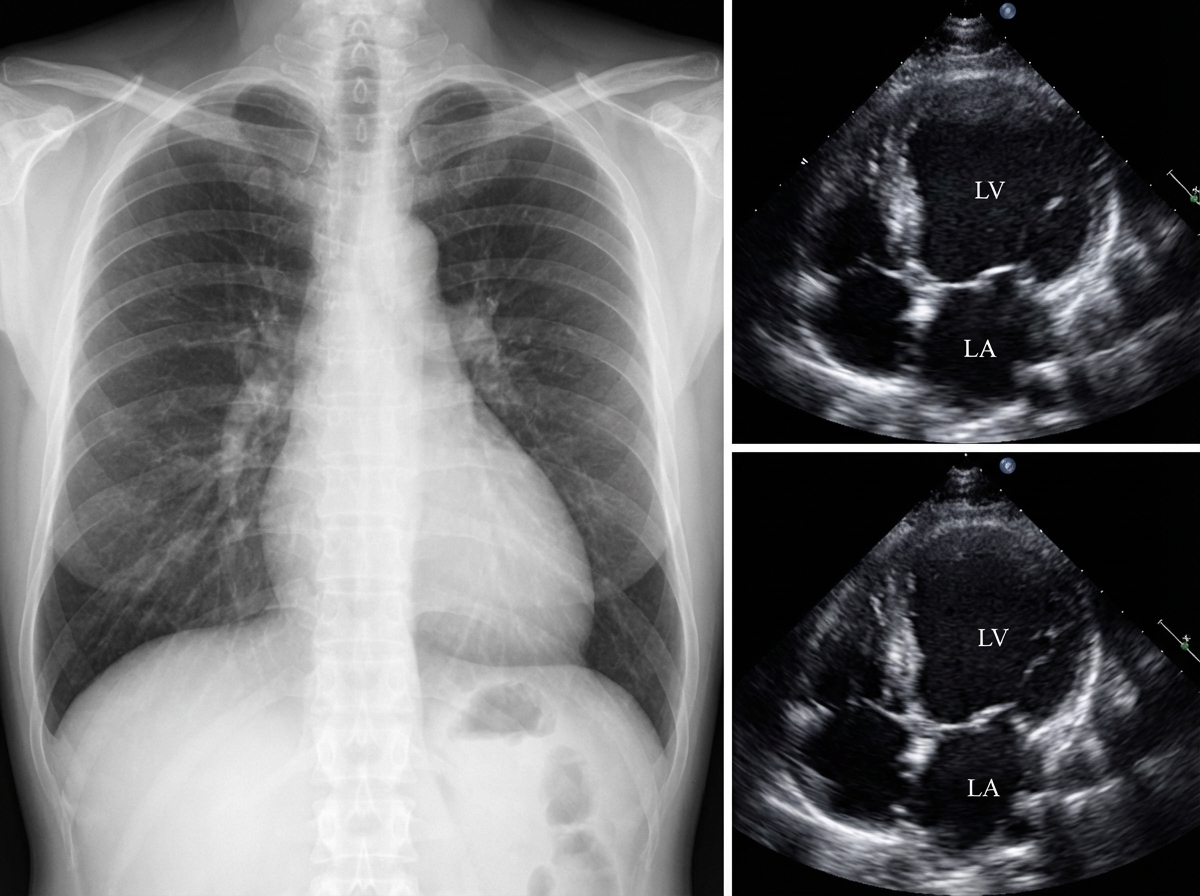
Which one of the following medications is most likely to be responsible for this appearance?
Which of the following is/are used in the hormonal therapy of breast carcinoma?
Which of the following is the main mechanism by which mechlorethamine exerts its cell killing?
All of the following statements about methotrexate are true EXCEPT:
Which of the following drugs cause metaphase arrest?
Which of the following agents is not a proliferation-independent agent?
Which of the following is an inhibitor of DNA synthesis?
Which antineoplastic drug is associated with very high cardiac toxicity?
Practice by Chapter
Principles of Cancer Chemotherapy
Practice Questions
Alkylating Agents
Practice Questions
Antimetabolites
Practice Questions
Antitumor Antibiotics
Practice Questions
Plant Alkaloids
Practice Questions
Topoisomerase Inhibitors
Practice Questions
Hormonal Agents
Practice Questions
Targeted Therapy
Practice Questions
Immunotherapy
Practice Questions
Management of Chemotherapy Side Effects
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app