
Anticancer Drugs — MCQs

On this page
Hand and foot syndrome can be caused by which of the following agents?
Pemetrexed, a drug useful in breast cancer, belongs to which of the following categories?
Which of the following anticancer drugs is excreted by the lungs?
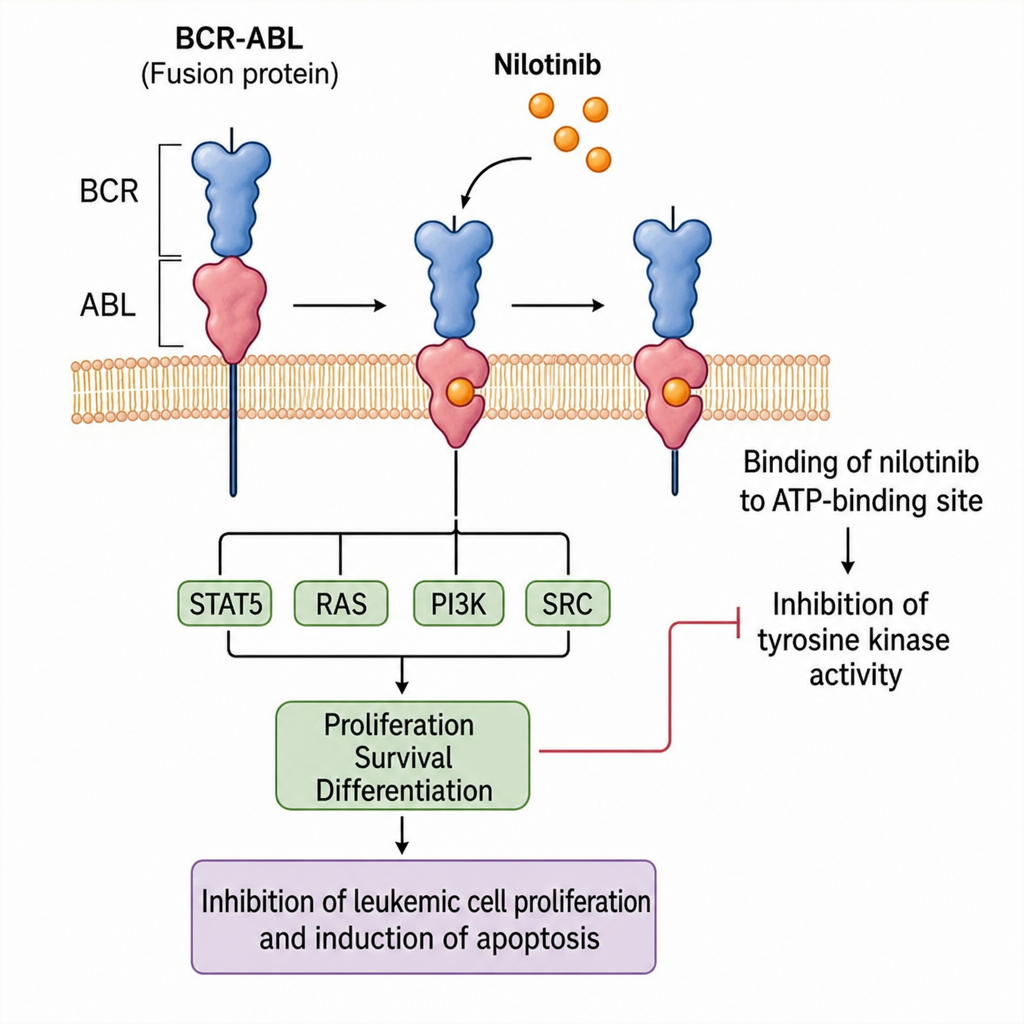
The figure shows the mechanism of action of which of the following drugs?
Which of the following antineoplastic drugs causes hepatotoxicity?
Stocking and glove neuropathy is seen in which of the following chemotherapeutic agents?
Which of the following immunosuppressive agents acts primarily by inhibiting helper T cells?
Which antimetabolite antineoplastic agent is used in the treatment of mesothelioma?
Coasting effect is seen with which of the following agents?
Which of the following anticancer drugs is least likely to cause nausea and vomiting?
Practice by Chapter
Principles of Cancer Chemotherapy
Practice Questions
Alkylating Agents
Practice Questions
Antimetabolites
Practice Questions
Antitumor Antibiotics
Practice Questions
Plant Alkaloids
Practice Questions
Topoisomerase Inhibitors
Practice Questions
Hormonal Agents
Practice Questions
Targeted Therapy
Practice Questions
Immunotherapy
Practice Questions
Management of Chemotherapy Side Effects
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app