
Upper Respiratory Tract Infections — MCQs

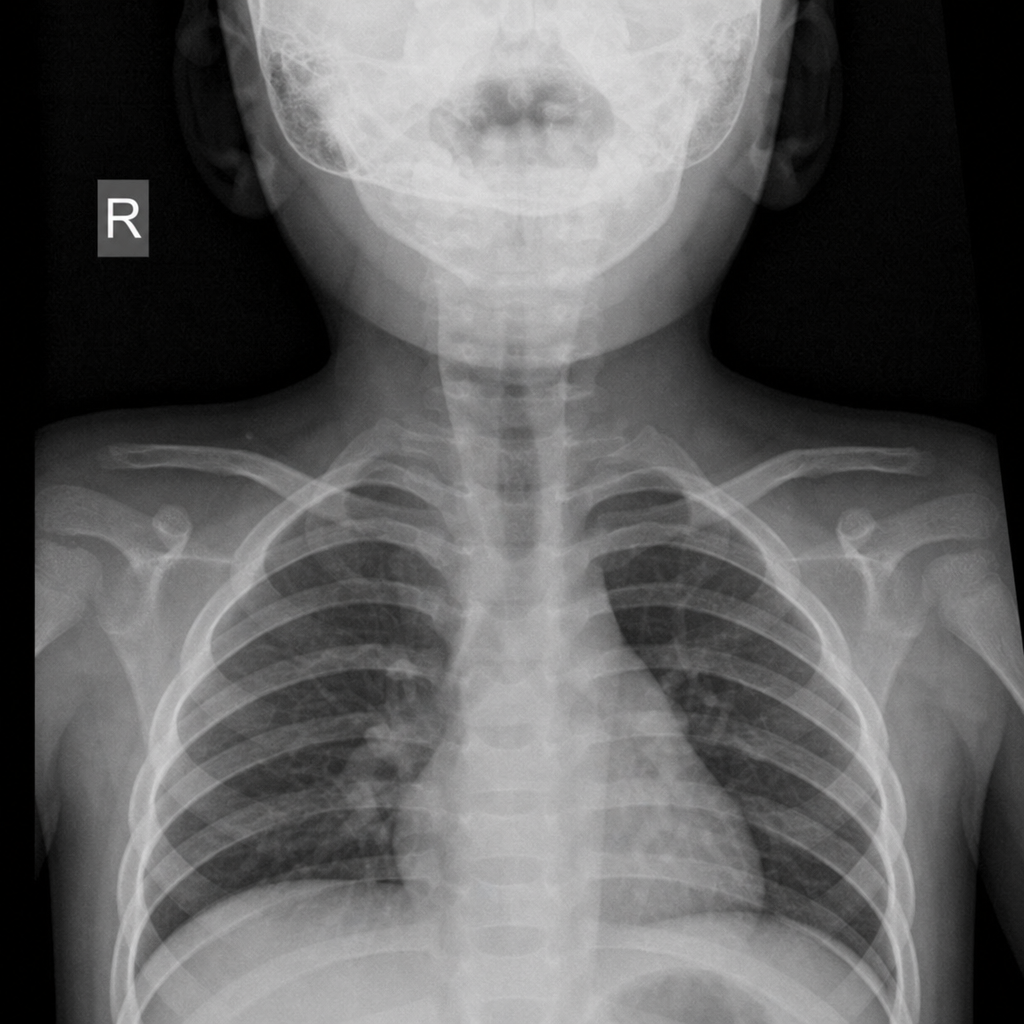
A 2-year-old child presented with the following x-ray finding. What is the most likely diagnosis?
4 year old male, recurrent URTI, has difficulty breathing, High arched palate, Failure to grow and impaired hearing, management is
A child presents with recurrent ear infections and conductive hearing loss. What is the most likely diagnosis?
A 4-year-old boy presents with low-grade fever, inspiratory stridor, and barking cough for the past 5 days. Examination reveals a hoarse voice, a moderately inflamed pharynx, and a slightly increased respiratory rate. His chest x-ray showed subglottic narrowing appearing like a steeple. Which among the following is not indicated in the treatment of this condition?
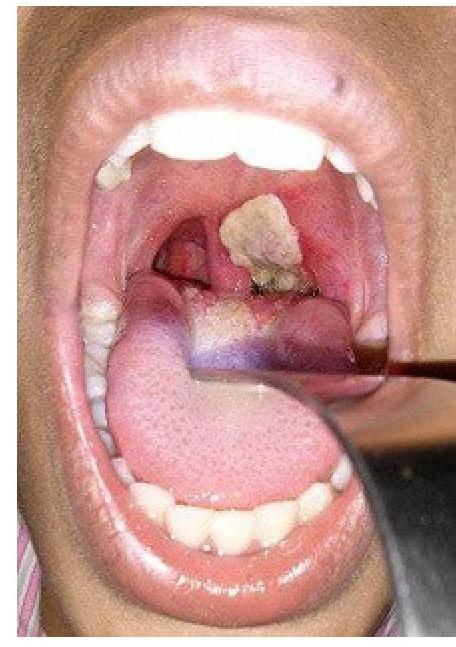
A patient presents with hoarseness of voice and a clinical condition as shown in the image. Identify the lesion:
Most dangerous sign in lower respiratory tract infection (LRTI) in children is:
Which of the following is not associated with primary ciliary dyskinesia?
A 2-month-old child with a birth weight of 2 kg presents with poor feeding, excessive sleepiness, and wheezing. What is the most likely diagnosis?
Which of the following conditions is most associated with digital clubbing in children?
A 24 month child, with a weight of 11 kg, has RR of 38 / min, chest indrawing, cough and fever. Management according to IMNCI?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app